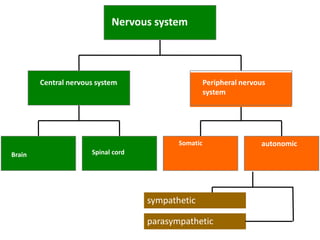
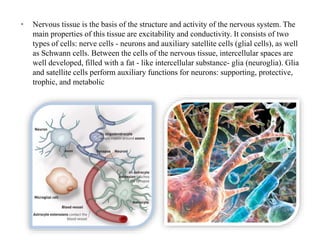
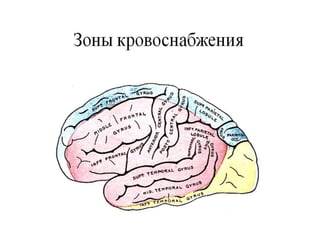
Neurology is a clinical discipline that developed in the 18th century to study the nervous system. It uses specialized investigation methods and has distinguished various neurological disorders. The nervous system regulates and coordinates the organism's activity and interaction with the external environment through interconnected nerve structures. It consists of the central nervous system (brain and spinal cord) and peripheral nervous system. The brain and spinal cord develop from ectoderm and mesoderm tissues during embryogenesis. Neurological examinations evaluate mental status, cranial nerves, motor strength, sensation, reflexes, coordination and gait to localize pathology. Neurological disorders are common causes of illness and can affect the brain, spinal cord or nerves.