Download to read offline









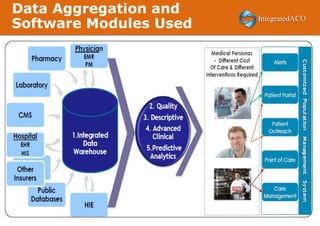














The document outlines the innovations and achievements of Integrated ACO, focusing on their advanced payment model and predictive analytics to improve patient care in underserved regions of West Texas. Key highlights include significant cost reductions, successful quality measure reporting, and the development of a predictive algorithm for preventable hospital admissions. The document also emphasizes the importance of personalized care coordination and the use of socio-economic data in enhancing healthcare outcomes.























































































