Downloaded 86 times



















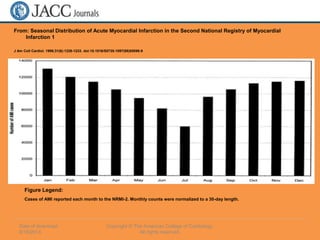




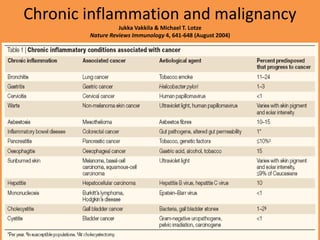
![Results
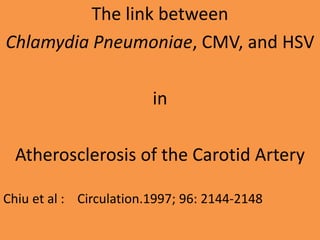
• C pneumoniae detected in 71%
(95% confidence interval [CI], 59.5% to 80.9%)
• CMV was detected in 35.5%
(CI, 24.9% to 47.3%)
• HSV-1 10.5%
(CI, 4.7% to 19.7%)](https://image.slidesharecdn.com/inflammation-140823155002-phpapp02/85/Inflammation-atherosclerosis-cancer-obesity-infections-dementia-depression-62-320.jpg)


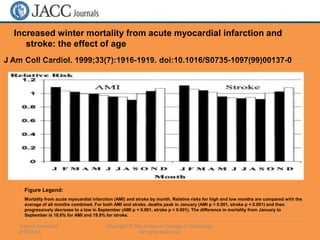
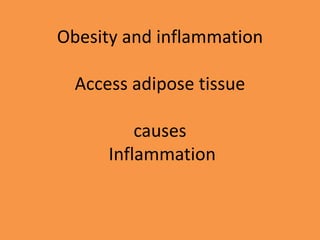
![Results
• Plaques were twice as common in
seropositives
40 of 1070 [3·7%] vs 64 of 3714 [1·7%]
• Intima-media thickening 4 times as common
(38 of 605 [6·3%] and 66 of 4179 [1·6%]](https://image.slidesharecdn.com/inflammation-140823155002-phpapp02/85/Inflammation-atherosclerosis-cancer-obesity-infections-dementia-depression-81-320.jpg)
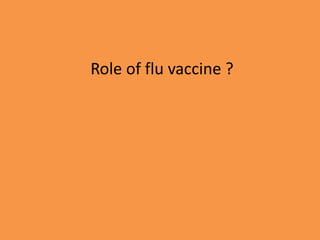
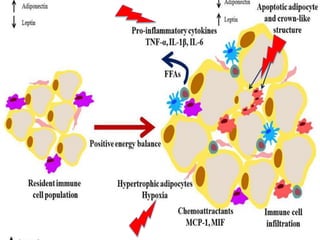
![Odds ratio and p values
• Increased risk of carotid-artery plaque
(odds ratio 1.92 [95% CI 1.56-2.38], p=0.002)
• Also with carotid intima-media thickening
(odds ratio 2.85 [2.28-3.57], p<0.0001)
Evidence was irrespective of known
atherogenic risk factors
---Ishizaka et al : Lancet. 2002;359:133–135](https://image.slidesharecdn.com/inflammation-140823155002-phpapp02/85/Inflammation-atherosclerosis-cancer-obesity-infections-dementia-depression-82-320.jpg)















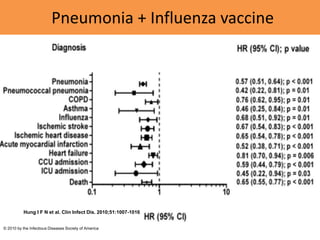
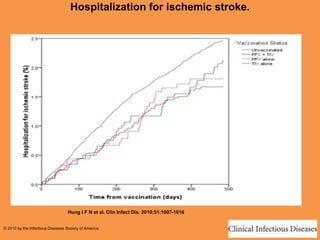
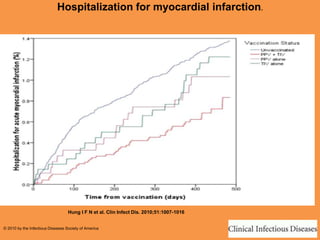
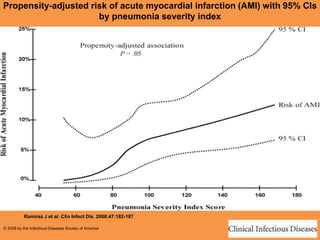
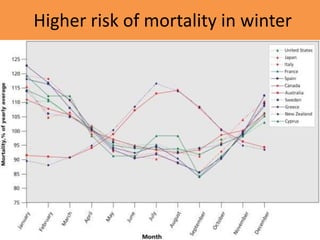
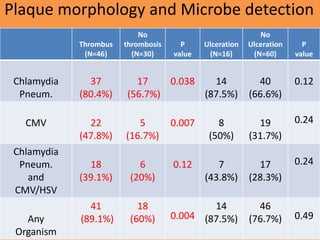
This document discusses inflammation and its role in various disease processes. Some key points include: - Inflammation plays a role in many leading causes of death like heart attacks and strokes. It is also involved in atherosclerosis and is considered an inflammatory process. - Acute infections can transiently increase the risk of heart attacks and strokes by enhancing inflammation. However, vaccines do not have this effect and may even help reduce risk. - Chronic infections like hepatitis C and periodontal disease are associated with higher levels of inflammation and worse plaque in arteries. This suggests they may exacerbate atherosclerosis. - Inflammation varies seasonally, with more heart attacks and strokes occurring in winter months when respiratory infection rates are highest













![Antibiotics bugs- us1 [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/antibiotics-bugs-us1autosaved-151215082823-thumbnail.jpg?width=640&height=640&fit=bounds)






































































