
Recommended
Recommended
More Related Content
Similar to Include a cover page and 1-2 pages of reflection regarding what ne
Similar to Include a cover page and 1-2 pages of reflection regarding what ne (20)
More from LizbethQuinonez813
More from LizbethQuinonez813 (20)
Recently uploaded
Recently uploaded (20)
Include a cover page and 1-2 pages of reflection regarding what ne
- 1. Include a cover page and 1-2 pages of reflection regarding what new learnings you've taken away from the week's activities, readings, videos, and other information you found noteworthy. For your Week 2 Journal consider the importance of having quality information to make decisions associated with creating and implementing strategies in your current place of employment. Required Resources Text There is not an official text for this course. Instead, there is a variety of selected reading materials that will be reviewed to ensure your success and meeting the learning objectives of the capstone. · Selected TRI Corporation Critical Equations for Business Leaders · Selected videos on strategy, developing an annual plan/budget, and variance analysis · Selected MBA materials in prior classe Articles Biery, M. E. (2013, December 22). What are your financial statements telling you? (Links to an external site.)Forbes. Retrieved from https://www.forbes.com/sites/sageworks/2013/12/22/understandi ng-financial-statements/#72daac5822b0 · The full-length version of this article is available through the Forbes.com website. This article provides information about analyzing trends associated with data used in financial analysis and will assist you in writing your Decision for Quarter One and also writing your First Quarter Quarterly Business Review this
- 2. week. How you think about the data and then develop decisions based upon your analysis drives overall performance. Accessibility Statement does not exist. Privacy Policy (Links to an external site.) Pal, N. (2015, April 9). Why financial dashboards matter, and five pointers to get you started (Links to an external site.). Forbes. Retrieved from https://www.forbes.com/sites/skollworldforum/2015/04/09/why- financial-dashboards-matter-and-five-pointers-to-get-you- started/#4f6e2f5f2520 · The full-length version of this article is available through the Forbes.com website. This article provides information about using financial dashboards used in graphical analysis of company financial data and will assist you in becoming familiar with tools used that help with analyzing information for your Decision for Quarter One and also writing your First Quarter Quarterly Business Review this week. Accessibility Statement does not exist. Privacy Policy (Links to an external site.) Sampson, L. (2015, March 13). Turning bean counters into difference makers: How corporate finance is changing with the times (Links to an external site.). Forbes. Retrieved from https://www.forbes.com/sites/oracle/2015/03/13/how- corporate-finance-is-changing-with-the-times/#1aaa9ab639d1 · The full-length version of this article is available through the Forbes.com website. This article provides information about using a wide variety of skills along with financial analysis that would be useful in digging deeper into the data generated by operations and will assist you in considering your Decision for Quarter One and also writing your First Quarter Quarterly Business Review this week. Accessibility Statement does not exist. Privacy Policy (Links to an external site.) Multimedia TriCorporation. (n.d.). Preparing your financial commitments: Guide to developing a budget as the leader of HISCO [Video
- 3. file]. Retrieved from https://qa.trisimulation.com/Simulation · This video provides information about the budgeting process that will be used within the Simulation and will familiarize you with what you will need to do in Week 2 for making budgeting decisions and submitting those decisions in the Simulation this week. The budget video will familiarize you Dashboards to be used in the Simulation. The video is found by clicking the (I) tab on the Simulation navigation bar and then clicking on the Supplementary Review materials tab. Accessibility Statement does not exist. Privacy Policy (Links to an external site.) Supplemental Materials Cadrain, S. (2020). Pre-tax net income chart explanationDownload Pre-tax net income chart explanation[Presentation slides]. [email protected] https://login.uagc.edu · This PowerPoint presentation covers information about how to analyze HISCO’s financial metrics specifically pre-tax and after-tax income. The presentation can be used as a tool to better understand the “Pre-Tax Income: Year Plan vs. Actual” graph located in the Grow Your Business” (GYB) simulation. Required Technology Website “Growing Your Business” – A Management Simulation. (https://uagc.tri-sim.com/canvas) · This website is where you will conduct your readings and work to complete the Decisions for Quarter One assignment and the First Quarter Quarterly Business Review (QBR) assignment. Accessibility Statement does not exist. Privacy Policy Mental Health Policy
- 4. Can access to mental health services be improved? A n estimated 58 million American adults, or one in four, suffer from a diagnosable mental disorder. Eleven million live with a serious mental illness, such as schizophrenia, bipolar disorder or major depression. Yet it can take years for some individuals to see a mental health professional. Some don’t want help, but the majority say treatment is often unaffordable. Others don’t know where to go for treatment or say that insurance coverage isn’t adequate. The contentious debate over gun control since the December massacre at Sandy Hook Elementary School has been accompanied by a less polarizing discussion about improving access to mental health care. Still, some proposals have split mental health advocates, in- cluding encouraging states to make court-ordered outpatient treat- ment easier to obtain. In addition, critics say new definitions of
- 5. mental illnesses will lead to over-diagnosis. Meanwhile, insurers and patient advocates struggle to interpret federal laws requiring equal treatment of mental and physical illnesses. I N S I D E THE ISSUES ....................427 BACKGROUND ................433 CHRONOLOGY ................435 CURRENT SITUATION ........440 AT ISSUE........................441 OUTLOOK......................443 BIBLIOGRAPHY................446 THE NEXT STEP ..............447
- 6. THISREPORT Demonstrators support a decision to charge police officers in Fullerton, Calif., in the beating death of a schizophrenic homeless man, 37-year-old Kelly Thomas. In January 2013 a judge declined to drop charges against the three officers, who have pleaded not guilty. Last year the city paid $1 million to Thomas’ mother to settle her wrongful death civil suit. CQResearcher Published by CQ Press, an Imprint of SAGE Publications, Inc. www.cqresearcher.com CQ Researcher • May 10, 2013 • www.cqresearcher.com Volume 23, Number 18 • Pages 425-448 RECIPIENT OF SOCIETY OF PROFESSIONAL JOURNALISTS AWARD FOR EXCELLENCE � AMERICAN BAR ASSOCIATION SILVER GAVEL AWARD 90th Anniversary 1923-2013 426 CQ Researcher THE ISSUES
- 7. 427 • Should states make iteasier to force the mentally ill into treatment? • Does the medical pro- fession define mental illness too broadly? • Do insurers treat mental and physical health equally? BACKGROUND 433 Rise of State HospitalsUrbanization and population growth gave rise to public mental hospitals after 1800. 433 Shift to Community CareAfter the 1940s, community mental health gained support. 434 Changing Federal PolicyThe Reagan administration and Congress sought to reduce disability payments. 437 Equal TreatmentThe Clinton and George W. Bush administrations sought to improve coverage. CURRENT SITUATION 440 Integrating CareProposed legislation would increase funding for men- tal health centers. 442 Mental Health in SchoolsPresident Obama wants better programs to identify students’ mental illness.
- 8. OUTLOOK 443 Legislation in LimboRecent mental health mea- sures have been tied to stymied gun proposals. SIDEBARS AND GRAPHICS 428 Government Funds MostMental Health Treatment Medicaid, Medicare and other programs paid 60 percent of the total in 2005. 432 Cost Deters Many FromTreatment Half say treatment is unafford- able. 434 Mental Health PrescriptionsSoar Medication orders more than doubled from 1996 to 2008. 435 ChronologyKey events since 1843. 436 Shortage of Mental HealthProfessionals Cited “It’s a huge problem, starting with the child mental health system.” 438 Police Trained to DealWith the Mentally Ill More than 2,700 crisis teams exist nationwide. 440 Young Adults Had MostSerious Mental Illness Nearly 8 percent of young adults had a serious mental illness in 2011.
- 9. 441 At Issue:Will the new mental-disorders manual lead to over-diagnosis? FOR FURTHER RESEARCH 445 For More InformationOrganizations to contact. 446 BibliographySelected sources used. 447 The Next StepAdditional articles. 447 Citing CQ ResearcherSample bibliography formats. MENTAL HEALTH POLICY Cover: Getty Images/Kevork Djansezian MANAGING EDITOR: Thomas J. Billitteri tj[email protected] ASSISTANT MANAGING EDITOR: Kathy Koch [email protected] SENIOR CONTRIBUTING EDITOR: Thomas J. Colin [email protected] ASSOCIATE EDITOR: Kenneth Jost STAFF WRITER: Marcia Clemmitt CONTRIBUTING WRITERS: Sarah Glazer, Peter Katel, Reed Karaim, Robert Kiener, Barbara Mantel, Tom Price, Jennifer Weeks SENIOR PROJECT EDITOR: Olu B. Davis
- 10. ASSISTANT EDITOR: Darrell Dela Rosa FACT CHECKER: Michelle Harris An Imprint of SAGE Publications, Inc. VICE PRESIDENT AND EDITORIAL DIRECTOR, HIGHER EDUCATION GROUP: Michele Sordi EXECUTIVE DIRECTOR, ONLINE LIBRARY AND REFERENCE PUBLISHING: Todd Baldwin Copyright © 2013 CQ Press, an Imprint of SAGE Pub- lications, Inc. SAGE reserves all copyright and other rights herein, unless pre vi ous ly spec i fied in writing. No part of this publication may be reproduced electronically or otherwise, without prior written permission. Un au tho rized re pro duc tion or trans mis - sion of SAGE copy right ed material is a violation of federal law car ry ing civil fines of up to $100,000. CQ Press is a registered trademark of Congressional Quarterly Inc.
- 11. CQ Researcher (ISSN 1056-2036) is printed on acid- free paper. Pub lished weekly, except: (March wk. 5) (May wk. 4) (July wk. 1) (Aug. wks. 3, 4) (Nov. wk. 4) and (Dec. wks. 3, 4). Published by SAGE Publica- tions, Inc., 2455 Teller Rd., Thousand Oaks, CA 91320. Annual full-service subscriptions start at $1,054. For pricing, call 1-800-818-7243. To purchase a CQ Re- searcher report in print or electronic format (PDF), visit www.cqpress.com or call 866-427-7737. Single reports start at $15. Bulk purchase discounts and electronic-rights licensing are also available. Periodicals postage paid at Thousand Oaks, California, and at additional mailing offices. POST MAS TER: Send ad dress chang es to CQ Re search er, 2300 N St., N.W., Suite 800, Wash ing ton, DC 20037. May 10, 2013 Volume 23, Number 18 CQRe search er
- 12. May 10, 2013 427www.cqresearcher.com Mental Health Policy THE ISSUES F our months after the massacre of six adults and 20 first-graders in Newtown, Conn., Senate Majority Leader Harry Reid, D-Nev., took to the floor of the chamber in early April to make a deeply personal plea for gun control legislation. “Sometimes people in a fit of passion will purchase a handgun to do bad things with it . . . even as my dad did — killed himself,” said Reid. 1 More than 38,000 people committed suicide in 2010, the latest year of available data, nearly half with guns. Nine in 10 who take their lives have a diagnosable mental illness, most often depression or a substance abuse disorder, ac- cording to the National Insti- tute of Mental Health (NIMH), a government research insti-
- 13. tute in Bethesda, Md. 2 After Newtown, Congress swiftly held hearings on gun control and on mental health care, despite the fact that the mental- ly ill account for a tiny fraction of gun crimes. While mental health advocates, researchers and scientists were wary about tying discussions about the frag- mented mental health care system to the gun control debate, they wel- comed the chance to advocate for bet- ter access to diagnosis, treatment and support services. “The burden of mental illness is enor- mous,” Thomas Insel, director of the NIMH, told lawmakers a month after Newtown. An estimated 58 million American adults, or one in four, suffer from a diagnosable mental disorder in any given year, and it takes a decade, on average, for them to make contact with a mental health professional, said Insel. More than 11 million of those adults suffer from serious mental ill- ness, including schizophrenia, bipolar disorder and major depression, and for them the average delay in treatment is five years. “That is five years of in- creased risk for using potentially life- threatening, self-administered treatments, such as legal or illicit substances, and even death,” said Insel. 3
- 14. Experts disagree on how to fix the country’s broken mental health sys- tem. Proposed legislation to improve access by pumping more federal Med- icaid money into community mental health centers, which treat more than 8 million low-income people a year, has some bipartisan support in Con- gress. But calls by families for states to make it easier to force the mentally ill into treatment are generating spirited opposition from civil liberties groups. Meanwhile critics complain that the American Psychiatric Association’s latest manual of psychiatric disorders, released this month, will do nothing to stop over-diagnosis of men- tal illness. The bipartisan Excellence in Mental Health Act would set new standards of care at com- munity mental health centers. It includes a list of mandated services and requires better in- tegration of treatment for men- tal illness and substance abuse; provides more Medicaid dol- lars for centers meeting those standards and funds the mod- ernization of existing centers and construction of new ones.
- 15. Sen. Debbie Stabenow, D- Mich., author of the Senate version of the bill, estimated that it would allow commu- nity mental health centers to treat an additional 1.5 million people each year. 4 “As we’ve listened to peo- ple on all sides of the gun debate, they’ve all talked about the fact that we need to address mental health treatment, and that’s what this does,” Stabenow said in mid-April as the Senate prepared to vote on the bill as an amendment to gun control legislation. 5 But gun control legislation failed, and the vote on the Excellence in Mental Health Act was shelved. “Today, our nation’s community men- tal health centers are simply stretched too thin and struggling to provide es- sential services,” said Linda Rosenberg, president and CEO of the Washington- based National Council for Communi- ty Behavioral Healthcare, a nonprofit association of 2,000 providers that sup- ports the bill. BY BARBARA MANTEL G e tt
- 17. r Janett Massolo of Reno, Nev., holds a photo of her daughter Shannon on March 22, 2013. Using her father’s handgun, Shannon committed suicide when she was 15 years old. Nine out of 10 people who take their own lives have a diagnosable mental illness, most often depression or a substance-abuse disorder. More than 38,000 people committed suicide in 2010, nearly half with guns. 428 CQ Researcher But Rosenberg criticized President Obama, whose fiscal 2014 budget, submitted to Congress in April, did not include funding for the proposed legis- lation. “I am extremely disappointed that the White House has not em- braced the Excellence Act, which would increase access and early intervention in communities around the country,” said Rosenberg. 6 The White House budget does call for $130 million in funding for other mental health proposals, including $55 million to train teachers and other adults to recognize the signs of men- tal illness in students and to help them refer students, when necessary, for services. The proposed budget also
- 18. includes $50 million in tuition sup- port to help train an additional 5,000 social workers, counselors and other mental health professionals to address critical shortages in many parts of the country. 7 Some professional groups said the money was welcome but far too little. “While we applaud President Obama’s budget proposal, it doesn’t come close to restoring the drastic cuts in funds for mental health services that have been imposed over the last several years,” said Robert Cabaj, chair of the Council on Advocacy and Government Relations at the American Psychiatric Association, a medical society in Ar- lington, Va. 8 Spending on mental health care to- taled $113 billion in 2005, before ad- justment for inflation, according to the latest available data, about twice the amount spent a dozen years earlier. (See graphic, above.) The money went mostly toward prescription drugs and outpatient treatment. Nevertheless men- tal health spending as a share of total health care outlays has been slipping; it was 6.1 percent in 2005, down from 7.2 percent in 1986. Private insurance has picked up an increasing portion of mental health ex-
- 19. penditures, accounting for 27 percent in 2005, up about 6 percentage points from a dozen years earlier. Patients’ out- of-pocket expenditures remained at roughly 12 percent, and the federal gov- ernment’s share was not much changed either, at about 28 percent. States’ share of mental health spending, however, dropped from 35 percent in 1993 to 30 percent in 2005 and is likely to have dipped further since. 9 The deep recession that officially began in December 2007 and ended in June 2009 took a huge toll on state finances, and states cut approximate- ly $5 billion in public mental health spending from 2009 through 2013, ac- cording to the National Association of State Mental Health Program Directors in Alexandria, Va. Over the same pe- riod, demand for publicly financed in- patient and outpatient mental health services rose 10 percent. “Those cuts have had a devastating impact on access to services for peo- ple,” says Ronald Honberg, national di- rector for policy and legal affairs at the National Alliance on Mental Illness (NAMI), an advocacy group in Ar- lington, Va. “It’s helped to further pre- cipitate a system that is responding to emergencies rather than doing ongo- ing care and prevention.”
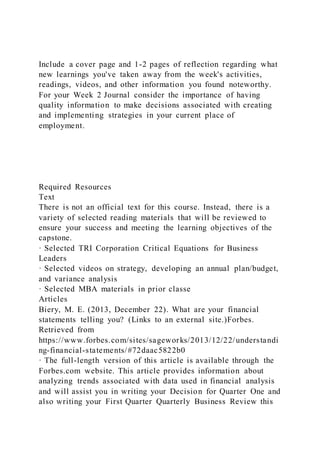
- 20. The number of state psychiatric hospital beds fell by about 4,500 — 9 percent of total capacity — between 2009 and 2012. Outpatient services have suffered as well. “In my own state of Arizona, virtually all state-only funded behavioral health services * have been dramatically reduced or eliminated over the last few years,” Laura Nelson, chief medical officer of the Arizona Department of Health, told Congress last year. “Over 4,600 children have lost behavioral health services. Nearly 6,300 adults lost ac- cess to substance abuse treatment services. 10 “Due to mental health cuts, we are simply increasing emergency depart- ment costs, increasing acute care costs and adding to the caseloads in our criminal and juvenile justice systems and correction systems,” said Nelson. MENTAL HEALTH POLICY Government Funds Most Mental Health Treatment Mental health spending in 2005, the latest year for which data are available, totaled $113 billion, about 60 percent of it paid by Medicaid, Medicare or other government sources. Private insurers paid nearly 30 percent. Mental health accounted for about 6 percent
- 21. of total health spending. Spending on Mental Health Treatment by Payer, 2005 2.6% Other private sources 27% Private insurance 29.8% State 28.4% Federal 12.2% Out-of-pocket Source: “National Expenditures for Mental Health Services and Substance Abuse Treatment, 1986-2005,” Substance Abuse and Mental Health Services Administration, Tables 74 & 75, pp. 201-202, http://hcfgkc.org/sites/default/files/documents/MHUS_ 2010_part3_508.pdf * Behavioral health services refers to mental health as well as substance abuse services.
- 22. May 10, 2013 429www.cqresearcher.com For example, in a survey of more than 6,000 hospital emergency depart- ments, 70 percent reported boarding psychiatric patients for hours or days, and 10 percent reported boarding such patients for weeks while staff looked for psychiatric beds. 11 And ac- cording to a recent report, the per- centage of inmates in New York City jails with mental health problems rose from 24 percent in 2005 to 33 per- cent in 2011. 12 Sheriff Brian Gootkin, who super- vises 48 deputies in Gallatin County, Mont. — an area twice the size of Rhode Island — blamed reductions in community mental health funding for a significant jump in psychiatric emer- gencies that his force must handle. “Every deputy that is diverted to the Montana State Hospital or even to a local hospital is not on patrol main- taining public order and deterring crime,” Gootkin complained. 13 The 2010 Patient Protection and Af- fordable Care Act — the sweeping health care system overhaul champi- oned by Obama — will add to the demand for mental health services as it extends health coverage to more than 30 million Americans, including an estimated 6 million to 10 million
- 23. with mental illness. Against that backdrop, here are some of the issues that lawmakers, advo- cates, mental health professionals and people with mental illness and their families are debating: Should states make it easier to force the mentally ill into treat- ment? On March 19, 2005, Roger Scanlan of Allentown, Pa., diagnosed with schiz- ophrenia and off his medications, killed his parents with a knife and then took his own life by cutting his throat. Five years later, his brother, Michael, testi- fied on behalf of proposed legislation in Pennsylvania to make it easier for courts to order outpatient treatment of the mentally ill. “I always knew when he wasn’t taking his meds,” Scanlan said of his brother. “He would become very pas- sionate about government, religion, and then he would believe that he was the second coming of Christ or Moses or some other biblical figure.” “Everyone from crisis, the Allentown Police Department, his doctors, they all knew the pattern. We, as a fami- ly, we couldn’t intervene to help him. We couldn’t get him off the street. We
- 24. were told that Roger had rights,” said Scanlan. “What rights did my mother and father have?” 14 The legislation died in committee in 2010. But since the Newtown mas- sacre, families and a prominent ad- vocacy group favoring easing rules for court-ordered treatment have renewed their campaign, testifying before Con- gress and at state forums. Civil liber- ties groups and other mental health advocates are strongly opposed, say- ing patients should not be forced into treatment. Forty-four states allow courts to order outpatient treatment of mental- ly ill people who have a history of not complying with treatment, which is sometimes referred to as assisted outpatient treatment or AOT. Most states require the person to be an im- minent danger to self or others. For example, in Pennsylvania, a court can’t order treatment unless the person com- mitted or tried to commit serious harm to self or others within the past 30 days. 15 But 10 states have less stringent cri- teria. For example, New York’s Kendra’s Law, named for a young woman pushed to her death in front of a subway train in 1999 by a schizophrenic man off his medications, does not require ev-
- 25. idence of recent harm. A New York court can order outpatient treatment for someone who is not complying with mental health treatment if non- compliance led to hospitalization or confinement in a mental health unit in a jail or prison at least twice in the last three years or to serious or at- tempted serious violent behavior in the past four years. 16 Doris Fuller, executive director of the Treatment Advocacy Center, a nonprofit based in Arlington, Va., wants states to model their laws on New York’s. Making it easier for courts to order outpatient treatment would help the small subset of people known in the mental health world as “frequent flyers,” says Fuller. “Many of them don’t acknowledge that they are ill or they don’t know that they are ill,” she says. Court-ordered treatment, which is monitored and carries penalties for failing to take re- quired medication, is needed to stabi- lize people until they voluntarily com- ply with treatment, she says. Many states rarely use their court- ordered outpatient treatment laws, and Fuller wants that to change as well. “California has a law similar to Kendra’s Law, but there are 58 counties in Cali- fornia and at this point, only one county has opted in and another has
- 26. a pilot program,” says Fuller. The same is true in Texas, she says, where courts in Dallas County have started using the state’s outpatient treatment law more frequently. “But then you have other counties that aren’t using it for whatever reason,” she continues. “The local mental health officials haven’t gotten on board, [and] there are con- cerns about what it will cost.” Patient-rights groups strongly object to looser criteria for or greater use of court-ordered outpatient treatment. “These laws [such as New York’s Kendra’s Law] are based on specula- tion,” says Debbie Plotnick, senior di- rector of state policy at Mental Health America, a national advocacy group for people with mental illness based in Alexandria, Va. Mental health dis- orders are episodic, she says. “People could have been in the hospital with- in the past three years and doing very well now in the community. You can- not say they are likely to be a danger to self or others.” 430 CQ Researcher The problem is not that the seri- ously mentally ill are refusing treat- ment, say Plotnick and others. “We have interventions that are effective for
- 27. the people that the Treatment Advo- cacy Center claims cannot be reached. The problem is that those interven- tions are not available for those who need them,” because of a lack of in- surance and funding, says Ira Burnim, legal director at the Washington-based Judge David L. Bazelon Center for Men- tal Health Law. These interventions include support provided by trained peers (people liv- ing successfully with mental illness); supported housing staffed by mental health workers; and so-called assertive community treatment or ACT, in which a team consisting of a psychiatrist, nurse, social worker, employment counselor and a case worker provides highly individualized services to an individual at home. “Another missing element of com- munity care that is sorely lacking around the country is the presence of a cri- sis center that can take people in for brief periods of time, arrange hospi- talization if needed and is available 24/7,” says Michael Hogan, New York state’s commissioner of mental health until retiring late last year. But Fuller says making treatment and support services more widely avail- able is not enough if people in crisis refuse to use them. “You could liter-
- 28. ally park people who are actively psy- chotic on the front door of the best service center in the country, and if they don’t think they are sick, they are not going to [voluntarily] walk through that door and access those services.” Plotnick rejects that argument. “I’m saying we should give people services upstream before they reach a crisis. We have to help them before they are in that stage,” she says. The largest and latest study of the impact of Kendra’s Law was published four years ago. It compared people’s experience under court-ordered out- patient treatment with their prior expe- rience, controlling for other factors. 17 “Overall, under assisted outpatient treatment, people were less likely to get hospitalized, more likely to receive appropriate medications for their con- dition, less likely to be arrested, and generally functioned better, with no apparent effect of feeling coerced,” as long as individuals were under court order for at least six months, says Mar- vin Swartz, a psychiatry professor at Duke University and the study’s prin- cipal investigator. The study found that these improvements were sustained once the court order expired.
- 29. “It makes sense because a Kendra’s Law order pushes you to the top of the line,” says Burnim. “They got bet- ter because they got access to much better services, not because of the court order.” In fact, unlike other states with as- sisted outpatient treatment, New York created a new stream of funding to ad- minister Kendra’s Law and also plowed money into expanding services for those who have a serious mental illness. But Swartz says his study showed that the court order itself conferred benefits. In one analysis, the researchers looked at people who were receiving intensive treatment from a team of professionals without a court order and with a court order. “We found that people under court order did better,” says Swartz. Hogan says there could be anoth- er explanation. Under court-ordered outpatient treatment, government watchers monitor the professional team delivering services, and, as a result, the quality of the treatment may have simply been better, he says. Does the medical profession de- fine mental illness too broadly? No laboratory tests exist to help
- 30. mental health professionals diagnose and treat mental illness. That absence is a huge disadvantage for psychiatry, according to Allen Frances, former chair of the psychiatry department at Duke University, and “it means that all of our diagnoses are now based on subjective judgments that are inherently fallible and prey to capricious change.” 18 As a result, the psychiatric profession has cast the net too broadly, capturing both those with mental disorders and those without, he says. Frances is an outspoken critic of the forthcoming fifth edition of the Diag- nostic and Statistical Manual of Men- tal Disorders (DSM), to be published this month by the American Psychiatric Association (APA). (See “At Issue,” p. 441.) First published in 1952, the DSM clas- sifies mental disorders, describing their symptoms and listing the number and duration of symptoms needed to make a diagnosis. The task force overseeing the newest iteration, the DSM-5, “gave their experts great freedom, and the ex- perts have used that freedom to do what experts always do, which is try to ex- pand their area of interest,” says Frances. But the manual’s supporters reject that view. “We developed DSM-5 by utilizing the best experts in the field
- 31. and extensive reviews of the scientif- ic literature and original research, and we have produced a manual that best represents the current science and will be useful to clinicians and the patients they serve,” said Dilip Jeste, APA president and chief of geriatric psychiatry at the University of Cali- fornia, San Diego. 19 The diagnostic manual has drawn criticism since its origin and has be- come increasingly controversial as its influence has grown. It “shapes who will receive what treatment,” said Mark Olfson, a Columbia University psychi- atry professor not involved in the re- vision. “Even seemingly subtle changes to the criteria can have substantial ef- fects on patterns of care.” 20 There have been plenty of not-so-subtle changes over the years, including an expansion of the number of diagnoses from 106 in the first edition to 297 in DSM-4. 21 MENTAL HEALTH POLICY May 10, 2013 431www.cqresearcher.com Critics of the version due to be pub- lished this month come from outside and inside the profession. Frances, in fact, was the chair of the task force for DSM-4, published in 1994. He points
- 32. to a new diagnosis included in the DSM-5 as just one example of what he says is wrong. It’s called Disruptive Mood Disregu- lation Disorder (DMDD), and it’s an attempt to reduce the number of young chil- dren who increasingly are diagnosed with bipolar disorder and medicated with pow- erful antipsychotic drugs. DMDD is a di- agnosis for irritable chil- dren who have been having “severe recur- rent temper outbursts that are grossly out of proportion in intensity or duration to the sit- uation.” 22 “The threshold for DMDD is high and children must meet several diagnostic cri- teria,” David Kupfer, chair of the DSM-5 task force and head of the psychiatry department at the University of Pittsburgh, says in an email. The outbursts must occur three times a week on average
- 33. and have been present for at least a year. But “in real life, it will be kids with tem- per tantrums who will get the diagnosis,” says Frances. “So instead of reducing the risk of exces- sive medication, I think this greatly in- creases it. If you want to attack the excessive diagnosis of bipolar disor- der in children, you should have big warnings in the bipolar section that this is being terribly over-diagnosed in kids, explain why and explain what should be done.” Several other changes to the diag- nostic manual also are raising hack- les. In the DSM-4, an individual griev- ing the loss of a loved one could not be diagnosed with major depressive disorder (MDD) unless symptoms per- sist for at least two months. For all other individuals, the threshold for a diagnosis of MDD is lower. Symptoms, such as sadness, loss of interest, loss of appetite, trouble sleeping and re- duced energy, need last only two weeks before a diagnosis can be made. The DSM-5 removes the exclusion for bereavement. Its elimination “shows that psychiatry has no idea how to
- 34. define what’s normal, what’s abnormal and how to differentiate between them,” said Allan Horowitz, author of The Loss of Sadness and a sociology pro- fessor at Rutgers University in New Jersey. “One of the essential ways we show our humanity is to grieve after the death of an intimate. Amazingly, psychiatry now sees this as a mental disorder.” 23 Psychiatrist Ronald Pies said such concern is mis- placed. “Grieving persons are not immune to major depressive disorder, and, indeed, bereavement is a common trigger” for it, said Pies, a professor at Tufts University School of Med- icine in Boston. Many mood disorder specialists think “the risk of over- looking MDD, with its high potential for suicide, far outweighs the less se- rious risk of ‘over-calling’ MDD,” said Pies. Besides, most experienced clinicians can tell the difference be- tween grief and major de- pression, he added. 24 But often, primary care physicians and pediatricians
- 35. are making the diagnosis, not specialists with years of training in mental illness, who are in short supply. “Primary care physicians look at the DSM with con- fusion,” says Peter Jensen, a child psychiatrist at the Mayo Clinic in Rochester, Minn. “If they use the DSM carefully, it will help them not treat someone as having Attention Deficit Disorder when they might ac- tually have anxiety or depression. 25 But if they’re rushed, they can’t do that, and that’s why we see over-diagnosis and over-treatment.” The DSM is not the problem, he says. “The scientists who come up Caseworker Cheryl Boone talks to a client during a therapy session at the Johnson County Mental Health Center in Shawnee, Kan., on Jan. 23, 2013. Proposed legislation to improve access to mental health treatment calls for pumping more federal Medicaid money into community mental health centers. A P P h o to /C
- 36. h a rl ie R ie d e l 432 CQ Researcher with the criteria have really struggled to make them as tight as possible,” Jensen says. Do insurers treat mental and physical health equally? When Congress passed the Mental Health Parity and Addiction Equity Act in 2008, it required group insurance plans sponsored by employers with 50 or more workers to put coverage of mental illness and substance abuse on an equal footing with physical health. But the Obama administration has yet to release the final rules imple- menting the law. “It took 12 years to pass that parity act, and four years later we still have no rules and there- fore no enforcement,” said James Ram-
- 37. stad, a former Republican congress- man from Minnesota and supporter of the bill. “It’s unconscionable.” 26 “A law without rules isn’t worth the paper it’s written on, and what that means is that insurance companies can continue to do business as usual,” said Patrick Kennedy, a former Democrat- ic congressman from Rhode Island and another of the law’s champions. 27 At a congressional budget hearing in April, U.S. Department of Health and Human Services (HHS) Secretary Kathleen Sebelius had only this to say: “We are committed to finalizing the rule this year and are in the process of doing just that.” 28 “Insurance plans have been work- ing hard on implementation,” based on an interim final rule the adminis- tration released in 2010, says Susan Pisano, spokeswoman for the Washington-based America’s Health Insurance Plans, the industry trade association. The indus- try supported the parity law, she says. The law is supposed to ensure that insurance plans don’t impose financial requirements — deductibles, copay- ments, out-of-pocket payments and co- insurance — for mental health care and substance abuse treatment that are more
- 38. restrictive than for physical health ben- efits. Parity also applies to treatment limitations. 29 For example, if an in- surance plan doesn’t limit the number of hospital days or out-patient visits for most physical care, it can’t place such limits on mental health care. Mental health advocates say insur- ers have done a pretty good job of getting those numerical limits in line but are falling down when it comes to scope of services. “We still continue to see wholesale exclusion of benefits on the behavioral health side that we don’t see on the medical/surgical side,” says Andrew Sperling, director of legislative advocacy for the National Alliance on Mental Illness. For example, plans will cover rehabilitation after a hospital stay for a stroke, but many won’t cover in- tensive day-therapy after hospitalization for substance abuse, he says. “We believe this violates the spirit of the law,” Sperling says. The Obama administration interim final rule men- tions parity for scope of services but has no binding requirements. Sperling hopes the final rule will make such requirements clear. The interim rule also states that in- surance plans must manage utilization of benefits evenly across mental health and physical health care. For example,
- 39. if a plan does not require prior autho- MENTAL HEALTH POLICY Cost Deters Many From Treatment About 11 million adults age 18 or older said in 2011 they did not receive treatment for a mental health problem. Many said treatment was unaffordable or that their insurance was inadequate. Nearl y 30 percent said they could handle their problems without treatment. Reasons for Not Receiving Mental Health Treatment, 2011 Source: “Results From the 2011 National Survey on Drug Use and Health: Mental Health Findings,” Substance Abuse and Mental Health Services Administration, 2012, www.samhsa.gov/data/NSDUH/2k11MH_FindingsandDetTables /2K11MHFR/NSDUH mhfr2011.htm 50.1% 0% 10 20 30 40 50 60 Fear of being committed and having to take medicine Might have negative effect on job Might create a negative opinion in community
- 40. Didn’t feel need for treatment Treatment wouldn’t help Confidentiality concerns/ not wanting others to find out Insurance wouldn’t cover any or enough treatment Didn’t have time Didn’t know where to find services Could handle problem without treatment Treatment unaffordable 28.8% 16.2% 15.1% 15% 13% 10.4% 8.5% 8.2% 7%
- 41. 7% May 10, 2013 433www.cqresearcher.com rization for medical and surgical ad- missions, then it can’t require prior authorization for mental health ad- missions, advocates say. The New York State Psychiatric As- sociation, along with three individu- als, filed a class action lawsuit in March against UnitedHealth Group, one of the country’s largest health insurers, charging that the company “improp- erly processed and discouraged claims for mental health and substance abuse,” says New York attorney Brian Hufford, the lead lawyer in the case. At its heart is a charge that the insurer requires pre-authorization for psychotherapy sessions but not for most outpatient medical care. “The only explanation I’ve seen is that for certain ancillary services, like physical therapy, they require pre- authorization, and so they say they can do it for mental health care,” says Hufford. But mental health is not an ancillary service like physical thera- py, he says. “We are committed to helping peo-
- 42. ple with mental health issues reach long-term recovery,” UnitedHealth Group said in a statement. “We have received the complaint and are cur- rently reviewing it.” 30 Comparing utilization review crite- ria across mental and physical health sounds straightforward, but it’s not as simple as comparing copays, says Pamela Greenberg, president and CEO of the Washington-based Association for Behavioral Health and Wellness, the trade association for the special- ized companies that insurers often hire — or own — to manage mental health benefits. “It’s a little bit like compar- ing apples and oranges,” she says. In addition, her members often can- not get the information they need from insurance plans to make these comparisons, says Greenberg. “We’re being asked to find out when does the medical plan require prior autho- rization and under what circum- stances, but there is no requirement [in the parity law] that [insurers] share it with us.” That lack of information also makes it difficult for consumers to know if their insurer is treating mental health benefits equitably. “The consumer is at
- 43. a complete loss,” said Julie Clements, deputy director of regulatory affairs at the American Psychiatric Association. 31 Advocates hope the final rule bet- ter clarifies what information insurers must share. “The delay really does re- flect the complexity of these issues and the need to get extensive input. People really had a lot to say about this,” says Gary Blau, chief of the Child, Adolescent and Family Branch of the federal Substance Abuse and Mental Health Services Administration. BACKGROUND Rise of State Hospitals B efore 1800, mentally ill people inAmerica were cared for at home or in their communities though chari- ty. But after 1800, rapid population growth, immigration, urbanization and growing geographic mobility upset those traditions, and an increasing number ended up in jail, in poorhouses, or in the few existing — and often over- crowded — mental hospitals, inspiring one woman’s crusade for better care. Dorothea Dix, a retired Boston teacher, visited a jail in 1841 to teach women prisoners and was horrified by the num- ber of mentally ill and the conditions in which they were kept. Galvanized by the experience, she visited jails and
- 44. poor houses across Massachusetts and addressed the legislature in 1843, de- nouncing “the present state of Insane Persons confined within this Common- wealth, in cages, closets, cellars, stalls, pens! Chained, naked, beaten with rods, and lashed into obedience!” 32 Dix helped convince lawmakers to expand the Worcester State Lunatic Asylum and, in the 1850s, build two new mental hospitals. Dix’s success in Massachusetts “launched her on a life- time career as an apostle for asylums,” wrote psychiatrist E. Fuller Torrey and his research assistant Judy Miller in The Invisible Plague. 33 During the 1840s and ’50s, a total of 23 public mental hospitals were built in 19 states, almost three times more than had been built in the pre- vious 20 years. Public officials and leg- islators supported the expansion of public mental hospitals in part because proponents promised the institutions “could cure insane individuals and therefore would ultimately save money,” wrote Torrey and Miller. 34 But most mental hospitals had more patients than they could handle ef- fectively, making it difficult to pursue time-consuming individualistic thera- py. By the early 1900s, “public facili- ties persisted as large and imperson-
- 45. al institutions characterized by a custodial attitude, meager allowances for active psychiatric treatment, limit- ed professional staff, and a depen- dence on untrained and unskilled per- sonnel,” according to health policy experts David Mechanic, Donna McAlpine and David Rochefort in Mental Health and Social Policy. 35 Shift to Community Care D uring the 1940s, several journal-ists published exposés of condi- tions in state mental hospitals. Life mag- azine published the lengthy article “Bedlam 1946” accompanied by “dra- matic and horrifying photographs” that “only added to its emotional impact,” wrote historians Gerald Grob and Howard Goldman in The Dilemma of Federal Mental Health Policy. At the same time, demoralized psy- chiatrists were abandoning mental in- stitutions for private or community 434 CQ Researcher MENTAL HEALTH POLICY practice, replaced by “foreign medical graduates with little or no training in psychiatry.” 36 Advocates for the men-
- 46. tally ill as well as lawmakers looking for cost savings began to embrace the idea of treating the seriously mentally ill as outpatients in their communities. In the 1950s, New York and Califor- nia passed laws establishing commu- nity mental health clinics. “The advent of the first generation of antipsychotic drugs was one of sev- eral factors contributing to the release of patients from state mental hospi- tals,” wrote health economists Richard Frank and Sherry Glied in Better But Not Well. “Chlorpromazine was the first medication to take the psychiatric world by storm, heralding the modern era of biological psychiatry.” It was first marketed in the United States in 1954 under the brand name Thorazine as a treatment for schizophrenia. Con- sidered widely effective, it came, how- ever, with serious neurologic side ef- fects, including rigidity and tremors. 37 In 1963, President John F. Kennedy signed into law the Mental Retardation Facilities and Community Mental Health Centers Construction Act. States could apply for federal grants to establish a system of community mental health cen- ters. The new centers were required to provide five essential services: inpatient hospitalization; partial hospitalization (in which patients live at home but come to the center up to seven days a week);
- 47. outpatient care; round-the-clock emer- gency care; and education and consul- tation services. The resident population in state and county mental hospitals fell from more than 500,000 in the 1950s to fewer than 40,000 by 2005. 38 Many patients were released back to families, group homes or single-occupancy residences to receive treatment locally, but oth- ers were simply shifted to nursing homes or general hospitals. “Federal programs offered an irre- sistible bargain to state administrators,” wrote Mechanic and colleagues. Medicare, created in 1965, covered men- tal health treatment for enrollees who entered general hospitals and private psychiatric hospitals; Medicaid, created at the same time to provide health care for the poor, paid a large share of men- tal health treatment costs for enrollees in general hospitals and nursing homes. “By directing patients away from pub- lic mental hospitals, then, the state could capture huge budgetary savings,” Mechanic and colleagues said. The result was a vast expansion in private nursing homes and private mental hospitals and a boom in specialized psychiatric and substance abuse units in general hospitals, they noted. “Over time, such facilities became the
- 48. main entry point for acute inpatient be- havioral health care.” 39 Meanwhile, the creation and con- struction of community mental health centers (CMHCs) proceeded slowly. A shortage of mental health profession- als was one problem. Another was the Vietnam War’s diversion of funding. A total of 2,000 mental health centers were supposed to be built by 1980, but the actual number was 754. “By then it had become abundantly clear that . . . CMHCs were not serving as replace- ments for traditional public mental hospitals,” according to Grob and Goldman. 40 In 1968 Congress expanded the role of the centers to serve substance abusers, children and older people. Grappling with a broader mission and tight re- sources, centers “chose to serve a great number of less impaired and lower-cost people rather than disproportionately allocating their budget to high-cost se- verely ill people,” wrote Frank and Glied. 41 In addition, the centers did not, and were not required to, coordinate continuing treatment and support for thousands of individuals being discharged each year from mental hospitals. By the end of the 1970s, the men- tal health system was a decentralized,
- 49. uncoordinated and bewildering array of institutions and practices: public and private psychiatric hospitals; nursing homes; residential care facilities; com- munity mental health centers, funded mostly by Medicaid but also by coun- ty, state and federal programs, Medicare and private insurance; outpatient and inpatient units in general hospitals; group homes; and client-run services. 42 Changing Federal Policy I n 1980, Congress passed the Men-tal Health Systems Act. The feder- al government would continue to issue grants to states, but now there would be performance contracts to ensure Continued on p. 436 Mental Health Prescriptions Soar More than 260 million prescrip- tions were filled in 2008 for mental health and substance- abuse medications for adults, more than twice the number in 1996. Antidepressants were the most prescribed drug. Other prevalent medications were for anxiety, psychosis and manic illnesses. Source: “Mental Health, United States,
- 50. 2010,” Substance Abuse and Mental Health Services Administration, 2010 Prescriptions Filled for Mental Health and Substance-Abuse Conditions Among Adults, 1996-2008 No. of Prescriptions (in millions) 105.4 0 50 100 150 200 250 300 200820021996 200.4 263.0 May 10, 2013 435www.cqresearcher.com Chronology 1840s-1950s States build public mental hos-
- 51. pitals; drugs for mental illness are developed. 1843 Activist Dorothea Dix denounces condition of the mentally ill con- fined in jails and poorhouses. 1860 Twenty-three public mental hospitals are built between 1840-1860. 1946 Life magazine publishes an exposé of deplorable conditions in many state mental hospitals. 1950s New York state and California pass laws establishing community mental health clinics as alternatives to hospitalization. 1954 Thorazine is marketed in U.S. to treat schizophrenia, heralding the modern era of biological psychia- try; considered widely effective, thorazine has serious neurologic side effects. 1956 The first tricyclic antidepressant to treat clinical depression is intro- duced. . . . More than 500,000 peo- ple reside in state and county men-
- 52. tal hospitals. • 1960s-1980s Federal laws empty public mental hospitals, as new drugs revolutionize treatment. 1963 Congress provides federal grants to states to establish community men- tal health centers to serve the de- institutionalized mentally ill. 1965 Newly created Medicare and Medic- aid pay for treating acutely mental- ly ill in general hospitals, private psychiatric hospitals and nursing homes; states shift many patients out of public mental hospitals into these facilities instead of into com- munities. 1968 Congress expands role of commu- nity mental health centers to serve children and the elderly. 1980 Only 754 community mental health centers have been built since 1963, far short of the pro- jected 2,000. . . . Congress passes
- 53. the Mental Health Systems Act. 1981 At President Ronald Reagan’s urging, Congress repeals the Mental Health Systems Act and reduces federal fund- ing to states for mental health care. 1983 Reagan administration purges 500,000 people from federal dis- ability rolls, a disproportionate number mentally ill. 1984 The Disability Benefits Reform Act prevents the government from ter- minating an individual’s disability benefits unless there is enough medical improvement to allow gainful employment. 1988 Prozac, the first selective serotonin reuptake inhibitor, or SSRI, is intro- duced for depression treatment. 1989 The first so-called atypical antipsy- chotic medication is introduced, followed by three more such drugs in the 1990s. •
- 54. 1990s-Present Insurance plans shift to man- aged care; government requires parity. 1990s Managed care plans adopted in effort to control rising health care costs. 1996 Mental Health Parity Act restricts large group health insurance plans from placing lower dollar caps on mental health benefits than on physical care. 2005 Resident population of state and county mental hospitals has fallen to 40,000. 2008 The Paul Wellstone and Pete Domenici Mental Health Parity and Addiction Equity Act signifi- cantly extends parity to insurance coverage of mental health and coverage of physical health in large group plans. 2010 Patient Protection and Affordable Care Act extends parity to individ- ual and small group plans pur- chased through newly created state insurance exchanges.
- 55. April 2013 Mental health legislation tied to gun control dies in the Senate when gun control bills fail to muster enough votes for passage; sponsors say they hope to reintro- duce mental health legislation later in the year. 436 CQ Researcher accountability. The role of communi- ty mental health centers was reaffirmed, with an emphasis on caring for the seriously mentally ill, and states could apply for grants to coordinate state and federal services. But upon taking office in 1981, Presi- dent Ronald Reagan reversed course and successfully persuaded Congress to repeal the act. Next, Congress signifi- cantly cut funding and then bundled the federal grants for community mental health centers and other federal fund- ing for mental health into a single lump sum given to each state annually with few strings attached. Finally, in response to a drastic expansion in the number of people receiving federal disability pay- ments, the Reagan administration began extensive in-person reviews in 1983 to
- 56. weed from the rolls those it decided were not permanently disabled. About 500,000 people lost their dis- ability payments, a disproportionate number of whom were mentally ill. The purge led to a public outcry, and in re- sponse Congress passed the 1984 Dis- ability Benefits Reform Act: The govern- ment could terminate benefits only if an individual’s medical condition improved enough to allow the person to return to gainful employment. The disability rolls have been increasing ever since, with the mentally ill the fastest growing group. 43 The late 1980s and ’90s also saw the development of new drugs to treat men- tal illness. A new generation of so-called atypical antipsychotic medications — MENTAL HEALTH POLICY Continued from p. 434 T ens of millions of Americans are living with mental ill - ness, but many are going without care, in part because of a shortage of qualified mental health professionals. The 2010 Affordable Care Act — the sweeping health care law championed by President Obama — will extend health cov- erage to an estimated six to 10 million individuals living with mental illness. 1 But experts cite a shortage of psychiatrists, clin-
- 57. ical psychologists, psychiatric nurses and specialized social work- ers to handle current demand, let alone any expansion. “It’s a huge problem, starting with the child mental health system,” says Ronald Honberg, national director for policy and legal affairs at the National Alliance on Mental Illness (NAMI), an advocacy group in Arlington, Va. “There is a severe short- age of child psychologists and psychiatrists around the coun- try, especially in rural areas.” (Child psychiatrists are medical doctors with special training in treating psychiatric problems in children and adolescents.) Dividing the number of children estimated to be suffering from serious emotional disturbance by the hours worked by practicing child psychiatrists yields, on average, one hour a year of attention per child. “You can’t even do an evaluation in an hour,” says Peter Jensen, a child psychiatrist at the Mayo Clin- ic in Rochester, Minn. “You can’t manage complex medications. You can’t do followup.” “The largest factor behind the shortage is the longer peri - od of education [required] to be a child psychiatrist,” says Kristin Kroeger Ptakowski, director of government affairs and clinical practice at the American Academy of Child & Adolescent Psy- chiatry, a professional medical association in Washington, D.C. (It takes six years of training after medical school to become a licensed child psychiatrist.) Moreover, practitioners say that once they are out of train- ing, the hours are long and the pay is relatively modest com- pared to other specialties. To accommodate children’s schedules, child psychiatrists often work afternoons and evenings, says
- 58. Harold Koplewicz, himself a child psychiatrist and president of the Child Mind Institute in New York, which conducts research and offers clinical services. “And if you are accepting insurance, you are paid for seeing the child. You are not paid for talking to school teachers or for counseling parents,” says Koplewicz. Students finishing a Ph.D. in psychology face their own hurdles. “There is a shortage of internship positions,” which is the cap- stone of clinical training and a requirement for a degree, says Cynthia Belar, executive director for education at the Washington- based American Psychological Association. Nearly 800 students out of roughly 4,500 could not find an internship in 2013, ac- cording the Association of Psychology Postdoctoral and Intern- ship Centers. 2 The Obama administration has proposed spending $50 mil - lion in fiscal 2014 to help train 5,000 new social workers, coun- selors, psychologists and peer professionals (individuals with mental illness who have successfully navigated the mental health system and can advise others). “It’s a step in the right direc- tion,” says Honberg. But some experts expressed concern when they learned that the money would be spent to train only master’s degree-level psychologists, social workers and counselors and not doctorate- level psychologists or psychiatrists as well. An administration official told The Washington Post that the aim is to help alle- viate the current demand for services. “We can’t take 12 years training doctors and post-docs to meet the need in 2014,” the official said. 3 But Kroeger Ptakowski says the administration’s strategy is short-sighted. “It’s unfortunate that it doesn’t include all men-
- 59. tal health professionals,” she says. “If these funds were avail - able now, I’m sure there would be many medical students who would be interested in going into child psychiatry.” Adds Belar: “An investment in one year of training [for psy- chology internships] for already-prepared doctoral students would seem as practical as supporting three-year programs.” Shortage of Mental Health Professionals Cited “It’s a huge problem, starting with the child mental health system.” May 10, 2013 437www.cqresearcher.com including clozapine, olanzapine, queti- apine and risperidone — have been shown in studies to be as effective as the older antipsychotic drugs in treating schizophrenia but with a reduction in the tremors and rigidity that made many people reluctant to stick with their drug regimen. However, the new drugs are more costly and have been associated with weight gain and diabetes. Tricyclic antidepressants were intro- duced in the 1950s and ’60s to treat major depression, but they had a long list of side effects, including drowsiness, dizziness, constipation, weight gain, headache and increased heart rate. The development of selective serotonin re-
- 60. uptake inhibitors, or SSRIs, beginning with Prozac in 1988, “transformed the treatment of depression,” according to Frank and Glied. SSRIs are of equal ef- ficacy as tricyclic antidepressants but are safer, better tolerated by patients and pose less danger from overdose, ac- cording to researchers. “These drugs en- tered both the medical mainstream, through their widespread use by pri- mary care providers, and the popular culture, with Peter Kramer’s best-selling book in 1993, Listening to Prozac,” wrote Frank and Glied. 44 Equal Treatment A s the cost of health care rose dueto an aging population, expensive new drugs and costly technological advances, such as the development of Koplewicz advocates increased spending to encourage pe- diatricians and family physicians to pursue advanced education in mental health because they do most of the diagnosing and treating of children with mental illness. “They must be better trained,” he says. Koplewicz proposes that primary care physicians who take an approved course in diagnosing and treating ADHD, ado- lescent depression, anxiety disorders and autism receive high- er reimbursement from Medicaid and possibly from private in- surance as well. Jensen founded the 5-year-old Reach Institute in New York,
- 61. which trains pediatricians and family doctors around the coun- try in child mental health during an intensive three-day inter- active program followed by six months of consultations with national experts. “We teach them pediatric psychopharmacology, but a little more than 50 percent focuses on assessment, diagnosis, form- ing a relationship with the family and how they can do this in 15 minutes every week or every other week until the fam- ily is stabilized,” says Jensen. “And we teach them when they should refer to a specialist,” mostly if they see signs of bipo- lar disorder or schizophrenia. Physicians also learn about cognitive behavioral therapy and other so-called evidence-based psychotherapy techniques so they can knowledgeably refer patients to counselors or psy- chologists. 4 Experts say better mental health care often requires a col - laborative approach in which a primary-care practice hires a social worker, counselor or psychologist on staff or as a con- sultant or contracts with a mental health group to treat adults or children. But there are barriers to making collaborative care work. One is financial. “The time that a pediatrician spends on the phone with a child psychiatrist discussing a case is not nec- essarily time that can be reimbursed by insurance,” says Darcy Gruttadaro, director of the child and adolescent ac- tion center at NAMI. Massachusetts legislators are working on a state law that would require insurers to pay for that time, she says. In addition, “The primary care physician may have a con- tract with one insurer and the mental health provider with an-
- 62. other,” says Wayne Lindstrom, president and CEO of Mental Health America, an advocacy group in Alexandria, Va. Anoth- er barrier may be something as mundane as office space. “It may not be available, and the primary care practice may be bound by a long-term lease” that would prevent the practice from moving into joint space with the mental health profes- sionals, says Lindstrom. Some of these challenges may be eased as the 2010 Af- fordable Care Act is phased in. Through a variety of pilot pro- grams and other enticements, the law encourages collaborative care and will experiment with paying integrated group prac- tices a lump sum for bundled services or for the annual care of each patient. However, many programs and incentives sanc- tioned under the new law have not been funded because of federal budget problems. — Barbara Mantel 1 For background, see the following CQ Researchers by Marcia Clemmitt, “Assessing the New Health Care Law,” Sept. 21, 2012, pp. 789- 812; “Health Care Reform,” June 11, 2010, pp. 505-528, updated May 24, 2011; and “Treating ADHD,” Aug. 3, 2012, pp. 669-692. 2 “2013 APPIC Match Statistics Combined Results: Phase I and Phase II,” As- sociation of Psychology Postdoctoral and Internship Centers, March 25, 2013, www.appic.org/Match/MatchStatistics/MatchStatistics2013Com bined.aspx. 3 Sarah Kliff, “Obama’s proposed budget to seek $235 million for new mental health programs,” The Washington Post, April 9, 2013, http://articles.washing
- 63. tonpost.com/2013-04-09/national/38403598_1_mental-health- services-gun-vio lence-health-insurance-coverage. 4 For background, see Sarah Glazer, “Treating Anxiety,” CQ Researcher, Feb. 8, 2002, pp. 97-120. 438 CQ Researcher sophisticated imaging machines, man- aged care emerged in the 1990s as a way to try to subdue the rising costs. Previously, an employer signed a contract with a single health insurance company to provide employees with a traditional indemnity plan — also known as a fee-for-service plan — that allowed individuals to use any doctor they chose and submit their bills to the insurer for partial reimbursement, typically 80 percent. Under managed care, employers often give employees a choice of plans. A health mainte- nance organization, or HMO, the old- est form of managed care, puts doc- tors on staff or signs contracts with medical practices to provide care for enrollees, who must use the physi- cians in the plan. A preferred provider organization (PPO), another form of managed care, is closer to a traditional fee-for-service plan. But enrollees are reimbursed at a lower rate if they use
- 64. doctors outside of the PPO network. In-network doctors have agreed to provide medical care at a discount. From the beginning, employers and general health plans chose to carve out coverage of mental health care and assign it to specialized behavioral health care companies. These compa- nies saved money by limiting the num- ber of days allowed for inpatient care, reducing prices paid to their network of mental health providers, limiting the number of outpatient visits and re- quiring preauthorization for treatment. The reliance on behavioral health care companies eventually spread from the private sector to Medicaid. Mental health advocates argued that the behavioral health care companies’ cost controls were discriminatory be- cause they were stricter than those for physical care. They lobbied Congress for parity, or equal treatment. Congress passed the Mental Health Parity Act of 1996, but its scope was limited. The act restricted the ability of group health insurance plans to place lower annual or lifetime dollar caps on mental health benefits than on med- ical and surgical benefits. But the act did not stop group plans from having higher copayments for mental health
- 65. care or from limiting the number of inpatient days or outpatient visits even when no such limits existed for medical or surgical care. The act also did not prevent group plans from dropping mental health coverage. It applied only to health plans sponsored by employ- ers with 51 or more workers, and it did not apply to health insurance cov- erage purchased by individuals. It also did not apply to treatment for sub- stance abuse. 45 The percentage of workers with dollar caps on mental health coverage fell substantially as a result of the law, according to researchers. But, contrary MENTAL HEALTH POLICY When the U.S. Justice Department cited the Portland,Ore., police department last September for a historyof excessive force against the mentally ill, city officials agreed to join a nationwide movement aimed at helping police better deal with people experiencing psychiatric problems. 1 As part of a settlement with the Justice Department, Portland formed a crisis intervention team within its police department to train law-enforcement personnel in how to respond to calls involving the mentally ill. “We all agree we can do better as a police bureau and as a community,” said Portland Police Chief Mike Reese. “This agreement will provide us a road map as we move forward.” 2 The first 50 police officers were selected for the specialized training in April.
- 66. More than 2,700 crisis intervention teams exist within law enforcement departments nationwide. The program originated in Memphis, Tenn., in 1988 and has spread to every state except Alabama, Arkansas and West Virginia. 3 “At least 10 percent of all police encounters involve some- one with a serious mental illness,” says psychiatrist Michael Compton, a professor of prevention and community health at George Washington University in Washington, D.C. The vast majority of these interactions don’t involve a high risk to pub- lic safety, he says. “They are minor infractions and misde- meanors, like loitering, subway fare evasions, things like that.” Crisis intervention teams are dispatched when police en- counter mentally ill individuals experiencing a psychiatric cri - sis. The teams aim to defuse the situation, prevent injury to the individual or police officers and decide whether the best course is arrest or mental health care. Police officers volunteer for the training. “A significant per - centage volunteer because someone they know and love suffers from mental illness,” says Jeffry Murphy, a 37-year veteran of the Chicago Police Department who supervised the creation of Chica- go’s training program for crisis intervention teams, which the city launched in 2004. Murphy has a son living with mental illness. During the 40-hour course, officers receive intensive in- struction on how to de-escalate a crisis situation, visit mental health facilities, speak with mental health professionals, inter - act with individuals with mental illness, role-play and ride along
- 67. with experienced team officers. Police dispatchers also receive special training. Police departments also are encouraged to forge relation- ships with mental health providers and advocacy groups in the community. Studies have shown that crisis intervention teams have a no- Police Trained to Deal With the Mentally Ill More than 2,700 crisis teams exist nationwide. May 10, 2013 439www.cqresearcher.com to advocates’ hopes, restrictions on in- patient days and outpatient visits for mental health care increased. 46 In 1999, President Bill Clinton’s sur- geon general, David Satcher, issued Mental Health — A Report of the Sur- geon General, a landmark analysis of the mental health field. It emphasized the need to understand mental illnesses as real, often disabling, health condi- tions and identified a range of effec- tive treatments backed by research that often had not been put into practice. In 2002, President George W. Bush formed the New Freedom Commission on Mental Health to study the nation’s mental health system and recommend improvements that would not increase spending. After a year of study, the com-
- 68. mission found that “recovery from men- tal illness is now a real possibility,” but that the mental health care system was a “patchwork relic — the result of dis- jointed reforms and policies.” 47 The report, though not a blueprint for action, defined several goals for transformation, including integration of mental and physical health care; empowerment of consumers and fam- ilies; increased early screening, as- sessment and referral; research-guided treatment; and improved access to and coordination of care. 48 When Bush announced the formation of the commission, he identified three barriers to mental health care: stigma, the fragmented delivery system and private health insurance plans’ often unfair treat- ment limitations and financial require- ments on mental health benefits. In- surance companies “must treat serious mental illness like any other disease,” the president said. 49 At the time, however, many con- gressional Republicans were opposed to so-called “mental health parity” for fear that it would drive up health care costs and discourage employers from offering coverage. But in 2008, after Democrats gained control of both hous- es of Congress, lawmakers passed the
- 69. Paul Wellstone and Pete Domenici Mental Health Parity and Addiction Equity Act. Like the 1996 law, it applied only to group plans, exempted plans spon- sored by small employers and allowed plans to drop mental health coverage. But it was far more ambitious than the previous law. It expanded parity by including deductibles, copayments, out-of-pocket expenses, co-insurance, covered hospital days and covered outpatient visits. It also expanded par- ity to substance abuse treatment. The 2010 Patient Protection and Af- fordable Care Act will eventually expand parity. Starting at the end of this year, individuals and employers with fewer than 100 employees — 50 or fewer in some states — can purchase health insurance through online exchanges ticeable impact on police officers. They are less inclined to stig- matize people with mental illness, know more about mental illness, display better de-escalation skills and are better able to refer people to mental health services, says Compton, who has studied crisis intervention teams. “And we know that these im- provements last beyond the training period.” But the ultimate goal of the teams is to reduce arrests and find help for those suffering from mental illness. Here the re- search is much thinner. “There have only been a couple of studies that I know of pertaining to arrest and referral deci-
- 70. sions,” says Compton. “In my own study, we did find evidence that [crisis intervention team] officers were less likely to make an arrest.” But training is only one of several factors driving arrest de- cisions, says Compton, “the big ones being the level of resis- tance of the subject and the level of violence potential.” No completed studies have examined the longer-term out- comes for individuals with mental health problems who encounter the intervention teams. Do most get appropriate care or end up in jail? Can they successfully live in the community, or do they have repeat encounters with police? A large, five-year study in Chicago designed to answer these questions is underway. Much depends on the availability and quality of mental health care providers and their relationships with the crisis intervention teams. Key, say researchers, is having a mental health facility nearby with a no-refusal policy. But a study of inter- vention teams across the country found that few programs had access to such a site and only about a third held “any type of formal agreement with mental health receiving facilities.” 4 State and city budget cuts have put pressure on crisis inter - vention teams. For example, Chicago has closed six of its 12 com- munity mental health clinics, promising that access to services wouldn’t be affected. But Murphy says that hasn’t happened. “We’re responding to more crisis calls because we have more people not linked to services,” he says. — Barbara Mantel
- 71. 1 For background, see Kenneth Jost, “Police Misconduct,” CQ Researcher, April 6, 2012, pp. 301-324. 2 Maxine Bernstein, “Portland mayor, chief, and Oregon U.S. Attorney an- nounce settlement on Portland police reforms,” The Oregonian, Oct. 26, 2012, www.oregonlive.com/portland/index.ssf/2012/10/portland_mayo r_chief_and_ orego.html. 3 CIT Center, The University of Memphis, http://cit.memphis.edu. 4 Michael T. Compton, et al., “The Crisis Intervention Team (CIT) Model of Collaboration Between Law Enforcement and Mental Health,” Advances in Sociology Research, Volume 9, 2011. 440 CQ Researcher MENTAL HEALTH POLICY operating in every state. Insurance plans offered through the exchanges must pro- vide mental health coverage and abide by federal parity rules. However, most Americans will continue to get health insurance through employer-sponsored plans that are not purchased through the exchanges. 50 The health law also expands Medicaid to anyone who earns less than 133 percent of the federal pover-
- 72. ty level (about $31,320 for a family of four), with the federal govern- ment footing most of the bill. 51 That could potentially extend health in- surance coverage to up to 10 mil- lion people with mental illness. How- ever, as of early May, 12 states were leaning toward opting out of Medic- aid expansion and another 13 were undecided. 52 CURRENT SITUATION Integrating Care A number of Democrats and Re-publicans in Congress are back- ing legislation they say will address the problems plaguing the nation’s mental health system. The Excellence in Mental Health Act would: • Increase funding for qualified com- munity mental health centers; • Increase access to an array of treat- ments and services that research has shown to be effective, including peer support, cognitive behavioral therapy, supported employment and support- ed housing; • Require community mental health centers to screen for physical health problems and collaborate with prima- ry care providers to give people with mental and addiction disorders med-
- 73. ical treatment and preventive care. “Integrating care is critically impor- tant,” says Honberg of the National Al- liance on Mental Illness. “We’ve had these two systems — mental health care and physical health care — operating far apart without talking to each other, and there have been huge consequences.” Honberg is referring to a 2006 re- port from the National Association of State Mental Health Program Directors that shocked many of those working in mental health care at the time. An- alyzing state data, researchers found that people with serious mental illness die, on average, 25 years earlier than the general population. While suicide and injury accounted for about one-third of those premature deaths, most were due to what the re- port called preventable medical condi- tions, such as cardiovascular, pulmonary and infectious diseases as well as dia- betes. Higher rates of smoking, alco- hol and intravenous drug use and poor nutrition put those with serious men- tal illness at greater risk for develop- ing those diseases than the general population. Homelessness, unemploy- ment, poverty, incarceration and social isolation also contribute to poor phys- ical health.
- 74. The new generation of antipsychotic drugs also plays a significant role. While they have far fewer neurologic side effects than older drugs, they are high- ly associated with weight gain, dia- betes, insulin resistance and other meta- bolic disorders. But equally important is the lack of access to primary care. 53 In response, four years ago the Substance Abuse and Mental Health Services Administration (SAMHSA) began issuing grants to com- munities that wanted to add primary care to services available at communi- ty mental health centers. SAMHSA cur- rently funds 93 such projects. “Just from being on medication for mental illness, I gained about 60 pounds,” said Gary Ward, who participates in a Washington County, Maine, program that provides primary and mental health care in one location. In two years, Ward has lost 38 pounds. “It’s given me my life back, it really has.” 54 Integrating care seems like a simple idea, but Kathleen Reynolds, vice pres- ident for health integration and well- ness promotion at the National Coun- cil for Community Behavioral Healthcare, says there are several challenges. Continued on p. 442
- 75. Serious Mental Illness in Adults Most Prevalent in Young Nearly 8 percent of adults ages 18 to 25 had a serious mental illness in 2011, compared with 6 percent of those 26 to 49 and 3 percent of those 50 and older (top). More than 6 percent of women had a serious mental illness, compared with about 3 percent of men (bottom). Source: “Results From the 2011 National Survey on Drug Use and Health: Mental Health Findings,” Substance Abuse and Mental Health Services Administration, 2012 Adults With a Serious Mental Illness, by Age and Gender, 2011 (Percent of Adults) 0 1 2 3 4 5 6 7 8%
- 76. 50+26 to 4918 to 25 0 1 2 3 4 5 6 7 8% FemaleMale 7.6% 6% 3% 3.4% 6.4% (Percent of Adults) no May 10, 2013 441www.cqresearcher.com At Issue: Will the new mental-disorders manual lead to over- diagnosis?yes
- 77. yes DR. ALLEN FRANCES PROFESSOR EMERITUS OF PSYCHIATRY, DUKE UNIVERSITY SCHOOL OF MEDICINE; FORMER CHAIR OF THE DSM-4 TASK FORCE; AUTHOR OF SAVING NORMAL WRITTEN FOR CQ RESEARCHER, MAY 2013 w e already are in the midst of a troublesome diagnos-tic inflation, and the revised edition of the Diagnos-tic and Statistical Manual of Mental Disorders (DSM-5) threatens to expand it into an even more harmful hyperinflation. The numbers are startling and scary. In any given year, 25 percent of the general population qualifies for a mental disorder; 50 percent will over their lifetime; and 20 percent take a psychotropic medicine. More people now die from overdoses caused by medicines prescribed by doctors than by street drugs sold by the cartels. In the last 20 years, rates of adult bipolar disorder have doubled, attention deficit disorder (ADD) has tripled, and autism and childhood bipolar disorder have grown a remarkable 40-fold. People don’t change quickly, but labels do. Small changes in how disorders are defined can result in large changes in who gets labeled. Diagnostic fashions are heavily influenced by drug-company marketing, which in the United States is fueled by enormous budgets and conducted with unprece- dented freedom from regulation. The ubiquitous advertising has successfully sold the misleading message that expectable problems of living are mental disorders that are caused by a chemical imbalance and require a pill solution. Illegal drug company marketing has led to multiple billion-dollar fines that
- 78. are not much of a deterrent given the enormous revenues generated by artificially created demand. The other major driver of diagnostic inflation is the fact that DSM diagnosis has become too important in decisions that determine eligibility for mental health care, school services and disability benefits. Except for autism, all the changes in DSM-5 will increase the rates of diagnosis — either by adding new disorders or reducing thresholds for existing ones. Expectable grief be- comes major depressive disorder; the normal forgetting of old age is mild neurocognitive disorder; worrying about a medical illness is somatic symptom disorder; overeating is binge eating disorder; temper tantrums are disruptive mood dysregulation disorder; and adult ADD will be so easy to diagnose that the already large illegal market of diverted stimulant drugs will be even harder to control. We should be tightening diagnostic standards, not loosening them. When we increase the resources devoted to the worried well who don’t need them, we deprive the really sick who desperately do.no DR. MICHAEL B. FIRST PROFESSOR OF CLINICAL PSYCHIATRY, COLUMBIA UNIVERSITY WRITTEN FOR CQ RESEARCHER, MAY 2013 n o one can say for sure what impact the new revisionof the American Psychiatric Association’s Diagnosticand Statistical Manual (DSM-5) will have on diag- nosis — the book isn’t out until this month, and its impact will slowly unfold over months, if not years. But it probably won’t lead to over-diagnosis. Anomalous rises in diagnostic rates are,
- 79. frankly, much more likely to be rooted in factors other than the diagnostic system. These include external pressures on clinicians to make diagnoses in a limited period of time; pressure from patients and families for quick fixes to complex problems, and pharmaceutical marketing influences. Psychiatric diagnosis is a complex process in which a trained clinician interacts with a patient to collect a psychiatric history, gathers corroborating information from family mem- bers, reviews medical records and laboratory findings and then determines the diagnosis by synthesizing this information and applying clinical judgment to the technical rules laid out in the American Psychiatric Association’s classification of mental disor- ders. When shortcuts are taken by not conducting a thorough evaluation or by ignoring the manual’s diagnostic rules, over - diagnosis and misdiagnosis, with its consequent overtreatment and mistreatment, can occur. The marked rise in the attention-deficit/hyperactivity disorder (ADHD) diagnosis over the past 20 years and the consequent escalation in stimulant prescriptions is a perfect illustration of the complex nature of this phenomenon. Under pressure from some parents, school systems and patients for a quick fix to improve attention and concentration or to get an edge over the competition, combined with heavy promotion by the pharma- ceutical industry of new drug formulations, many clinicians applied the ADHD label inappropriately. They did so to justify their decision to write a prescription for stimulants without having conducted a proper symptomatic or functional assess- ment or having determined that the requirements for the diag- nosis, as laid out in the DSM, were met. For example, there should be clear evidence of clinically significant impairment in social, academic or occupational functioning. The best hope to combat misdiagnosis of any kind would
- 80. be an intensive educational campaign promoting comprehensive diagnostic evaluation using accepted scientific methods. Sug- gesting that the DSM classification itself is the main reason for over-diagnosis ignores the fact that psychiatric diagnoses do not simply exist in the abstract. They are tools used by clini- cians to foster communication and to improve clinical care. Diagnoses are only as good as the people making them. 442 CQ Researcher “One is financing,” says Reynolds. Com- plicated Medicaid and Medicare billing rules don’t make it easy to bill for both primary and mental health care from one location. Another challenge is confiden- tiality. Federal and state confidentiality rules and regulations can make it difficult for a mental health provider and a pri- mary care provider work- ing together onsite to share information if they are from different agen- cies. “Yes, you can do it by getting every person to sign a release, but it is a burden to make sure those releases are up to date and cover all the in- formation,” says Reynolds. Yet another challenge
- 81. is cultural and organiza- tional, she says. Mental health professionals typ- ically spend long peri- ods with individuals and get paid to do so. Pri- mary care providers get paid per encounter, no matter how long the visit, so “the pace of the work in primary care is much faster,” says Reynolds. Combining the two types of care in one visit can be a challenge. “You don’t want to have a per- son come in and spend two or three hours,” says Reynolds. “In most cases, it’s the behavioral health side that modifies its prac- tices, coming up with shorter interventions.” Mental Health in Schools P resident Obama has called forspending $55 million in fiscal 2014 to reach 750,000 young people through programs to identify mental illness in schools and refer them to treatment when needed. “If you think about adult mental illness, about 50 percent of all those illnesses can be traced and man-
- 82. ifest by the age of 14, and three-quar- ters manifest by the age of 24,” says Blau of SAMHSA, which would fund the effort if it survives congressional budget negotiations. “That’s why we need to emphasize prevention in early childhood.” But schools do not have enough qualified staff members to work as part of mental health teams, according to groups representing such professionals. Jill Cook, assistant director of the Alexandria, Va.-based American School Counselor Association, says there cur- rently are 471 students per school counselor nation- wide — far too many. “Even though there has been im- provement over the past several decades, our asso- ciation’s recommendation is one school counselor for every 250 students,” she says. In addition, many states don’t require school nurs- es. As a result, the cover- age varies widely, from a high of 4,411 students per school nurse in Michigan in 2011 to a low of 396 in
- 83. Vermont. 55 “In the North- east the ratios are more re- alistic and safe for kids, but as you go further South and West, there often is no requirement for school nursing, and the ratios get larger,” says Linda Davis- Alldritt, president of the Na- tional Association of School Nurses, based in Silver Spring, Md. Obama’s plan calls for bringing a program called Mental Health First Aid into schools to train teachers, school security officers and even front-desk personnel to recognize the signs of mental illness in youngsters. Introduced in the United States in 2008 and modeled after a program in Australia, Mental Health First Aid is a 12-hour interactive training course de- signed to help the public identify, under- MENTAL HEALTH POLICY Continued from p. 440 University of Maryland junior Grace Freund studies to become a volunteer at the school’s student-run Help Center, which works with students dealing with mental health crises. Of the estimated
- 84. 58 million American adults with a diagnosable mental disorder, more than 11 million have a serious mental illness, such as schizophrenia, bipolar disorder or major depression. G e tt y I m a g e s/ T h e B a lt im o re S u n /M C T /K e v in R e
- 85. ct o r May 10, 2013 443www.cqresearcher.com stand and respond appropriately to signs of mental illness and substance use disorders. More than 120,000 peo- ple have been trained since its in- ception in the United States. “It has the potential to normalize mental illness in the public eye, not unlike physical illness,” says Wayne Lindstrom, president and CEO of Men- tal Health America. Mental Health First Aid recently mod- ified its program for use in schools, reducing it to eight hours and alter- ing the content to better reflect signs and symptoms in young people. Two school districts — in McAllen, Texas, and Tulare County, Calif. — have signed on so far. “We don’t teach people how to diagnose or treat mental illness,” says Bryan Gibb, director of public ed- ucation at the National Council for Community Behavioral Healthcare, which helps run the program. Nor do Mental Health First Aid instructors sim- ply give teachers a list of warning signs with instructions: “If you see these,
- 86. pick up the phone,” says Gibb. “There would be so many false alarms.” Instead, instructors show teachers how to de-escalate a crisis, such as when someone threatens suicide or hallucinates. But instructors spend the most time teaching adults how to have a nonjudgmental conversation with stu- dents and “refer them to professional help if necessary,” says Gibb. That referral doesn’t happen with- out permission from a parent or guardian, he adds. Gibb says the organizers also rec- ognize the risk that teachers might see signs and symptoms of mental disor- ders, such as depression, anxiety or an eating disorder, where there are none. “We tell teachers . . . we really want you to be aware of that bias,” says Gibb. So far, there have been no studies of Mental Health First Aid’s effectiveness in schools, but Gibb says studies are planned. SAMHSA says it will monitor the pro- gram’s impact on teachers and students if Congress authorizes funding. OUTLOOK Legislation in Limbo S enators sponsoring mental health leg-islation planned to piggy-back on the
- 87. gun control bill that was up for a vote in the Senate last month, offering their proposals as amendments. During two days of tense voting on the gun bill, the Senate overwhelmingly passed the Men- tal Health Awareness and Improvement Act, which would reauthorize several fed- eral programs, such as suicide preven- tion, and fund a new initiative to bring Mental Health First Aid into schools. But when the gun bill died, so did the Men- tal Health Awareness law, at least for now. The gun bill’s death in the Senate also has left the more heavily lobbied Excellence in Mental Health Act in limbo. It never even came up for a vote as an amendment. Now its Sen- ate sponsors and mental health advo- cates must adjust their strategy. “We’re pushing for co-sponsors, and the more co-sponsors we get the more likely it is that Senate Majority Leader Harry Reid will give us a vote,” says Sperling of the National Alliance on Men- tal Illness. Sperling says NAMI is prepar- ing for two possibilities: that the Senate gets a second crack at voting on gun legislation or that the mental health act’s sponsors will offer it as amendment to some other bill. “We have our members and affiliates calling senators, writing in, emailing, you name it,” he says. The lead sponsors of the Excellence
- 88. in Mental Health Act will decide the ultimate strategy. “I think there’s a re- ally good opportunity we can still get this done. It should not be dependent on gun legislation,” Sen. Roy Blunt, R- Mo., told Politico after the gun bill was pulled from the Senate floor. “I feel very confident we will get a vote at some point,” added Michigan Demo- crat Debbie Stabenow. 56 Without a federal law, action on men- tal health is left to the states. Some states — such as Pennsylvania and Wisconsin — are considering restoring some of the money cut from mental health budgets. But Joel Miller, senior director of policy and healthcare reform at the National Association of State Mental Health Pro- gram Directors, says he doesn’t think most states will restore mental health money. “There are Midwestern industri- al states like Illinois and Michigan that have not funded their public pensions properly, so they’re going to take it out on the health care side.” The most important action states can take right now, says Miller, is to sign on to the Affordable Care Act’s Medic- aid expansion program, which could extend health care coverage to as many as 10 million additional people living with mental illness. “That will bring new federal monies into state budgets for treating people with mental illness,” he
- 89. says. In the first three years of the ex- pansion, beginning in 2014, the feder- al government will cover 100 percent of the costs for expanded enrollees and then 90 percent after that. But as of early May, only 20 states had commit- ted to Medicaid expansion, with an- other six leaning toward it. 57 Several Republican governors have spoken out against expanding Medic- aid, including Gov. Rick Perry of Texas. “Texas will not be held hostage by the Obama administration’s attempt to force us into the fool’s errand of adding more than a million Texans to a broken system,” Perry said in early April. 58 The Southern-most states from Texas to North Carolina, with the ex- ception of Florida, are leaning toward opting out of Medicaid expansion. So are Idaho, Missouri, Oklahoma, Mon- tana and Alaska. 59 Advocates are working hard to con- vince legislatures and governors in those states to change their minds. “There are so many people who have no ac- cess whatsoever to health care and who have extreme needs,” says Plotnick of 444 CQ Researcher Mental Health America. “The Medicaid
- 90. expansion would reach those folks who have nothing.” Notes 1 Ginger Gibson, “Harry Reid cites father’s suicide in gun debate,” Politico, April 9, 2013, www.politico.com/story/2013/04/harry-reid- gun-debate-father-suicide-89805.html. 2 “Web-based Injury Statistics Query and Re- porting System,” Centers for Disease Control and Prevention, www.cdc.gov/ncipc/wisqars; “The Numbers Count: Mental Disorders in Amer- ica,” The National Institute of Mental Health, www.nimh.nih.gov/health/publications/the- numbers-count-mental-disorders-in-america/ index.shtml. 3 Thomas Insel, testimony before the Com- mittee on Health, Education, Labor, and Pen- sions, U.S. Senate, Jan. 24, 3013, pp. 2, 4, www. help.senate.gov/imo/media/doc/Insel.pdf; “The Numbers Count: Mental Disorders in Ameri- ca,” op. cit. 4 Debbie Stabenow, “Strengthening Mental Health Services,” www.stabenow.senate.gov/? p=issue&id=80. 5 Jeremy W. Peters, “In Gun Debate, No Rift on Better Care for Mentally Ill,” The New York Times, April 12, 2013, www.nytimes.com/2013/ 04/13/us/politics/senators-make-bipartisan-push- for-mental-health-care.html?pagewanted=all&_ r=0. 6 “Crucial Mental Health Legislation to be Considered Next Week,” National Council for Community Behavioral Healthcare, April 11, 2013, www.thenationalcouncil.org/cs/press_
- 91. releases/crucial_mental_health_legislation_to_ be_considered_next_week. 7 “Fiscal Year 2014, Budget in Brief,” De- partment of Health and Human Services, p. 41, www.hhs.gov/budget/fy2014/fy-2014- budget-in-brief.pdf. 8 “Obama Includes Mental Health Funding Increase in Budget Proposal,” Psychiatric News Alert, April 10, 2013, http://alert.psychiatricnews. org/2013/04/obama-includes-mental-health- funding.html. 9 “National Expenditures for Mental Health Services and Substance Abuse Treatment, 1986- 2005,” Substance Abuse and Mental Health Services Administration, Tables 74 & 75, pp. 201-202, http://hcfgkc.org/sites/ default/files/ documents/MHUS_2010_part3_508.pdf. 10 Laura Nelson, “Opening Presentation: Impact of the State Budget Crisis and Treatment Gap on the Public Substance Abuse and Mental Health System,” National Association of State Mental Health Program Directors, March 22, 2012, pp. 6-7. 11 Ibid., pp. 4, 7. 12 “Improving Outcomes for People with Mental Illnesses Involved with New York City’s Criminal Court and Correction Systems,” Jus- tice Center of the Council of State Govern- ments, December 2012, p. 1, http://consensus project.org/jc_publications/improving-outcomes- nyc-criminal-justice-mental-health/FINAL_NYC_ Report_12_22_2012.pdf. 13 “Proceedings on the State Budget Crisis and the Behavioral Health Treatment Gap: The Impact on Public Substance Abuse and Mental Health Treatment Systems,” National