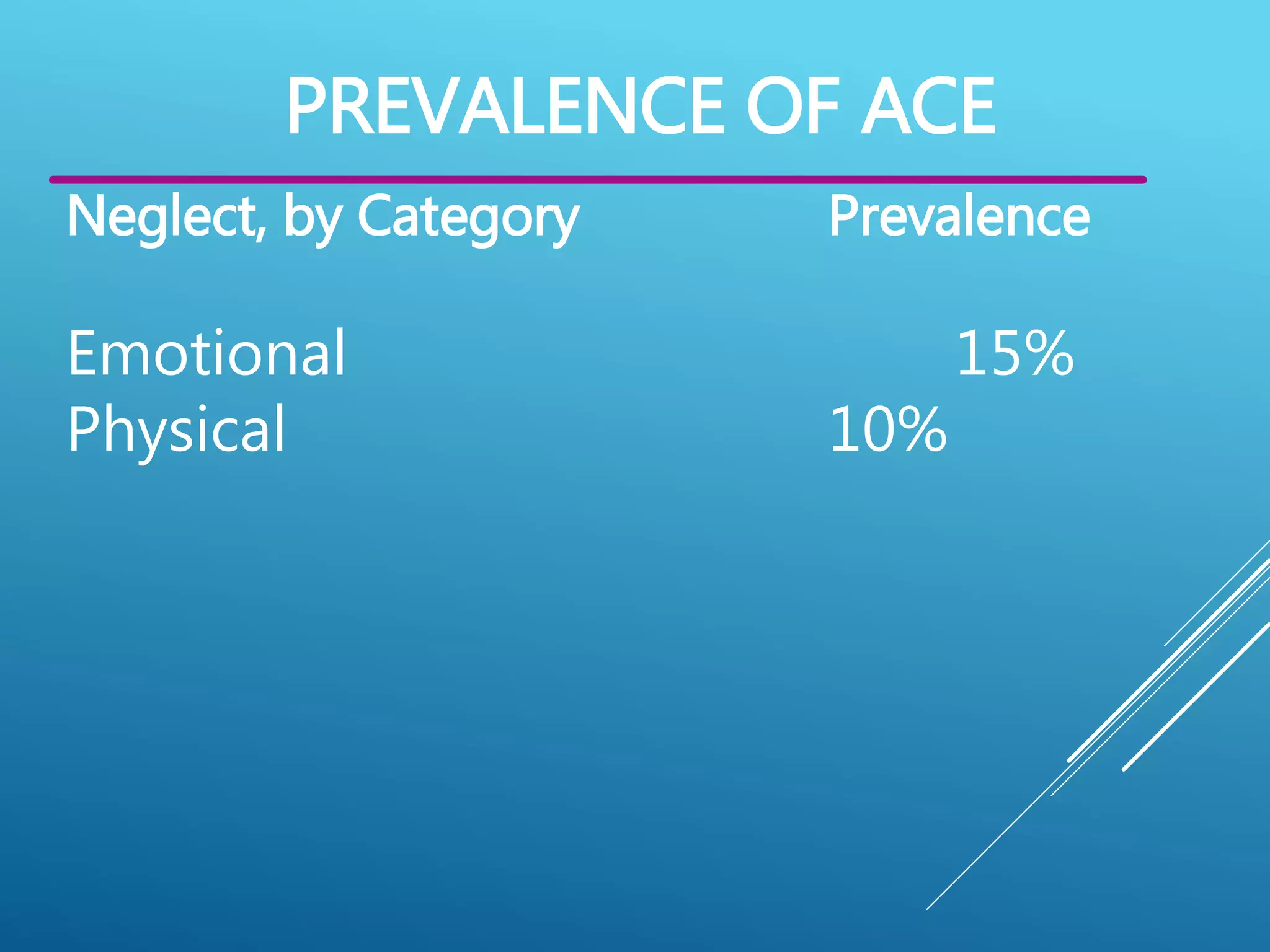
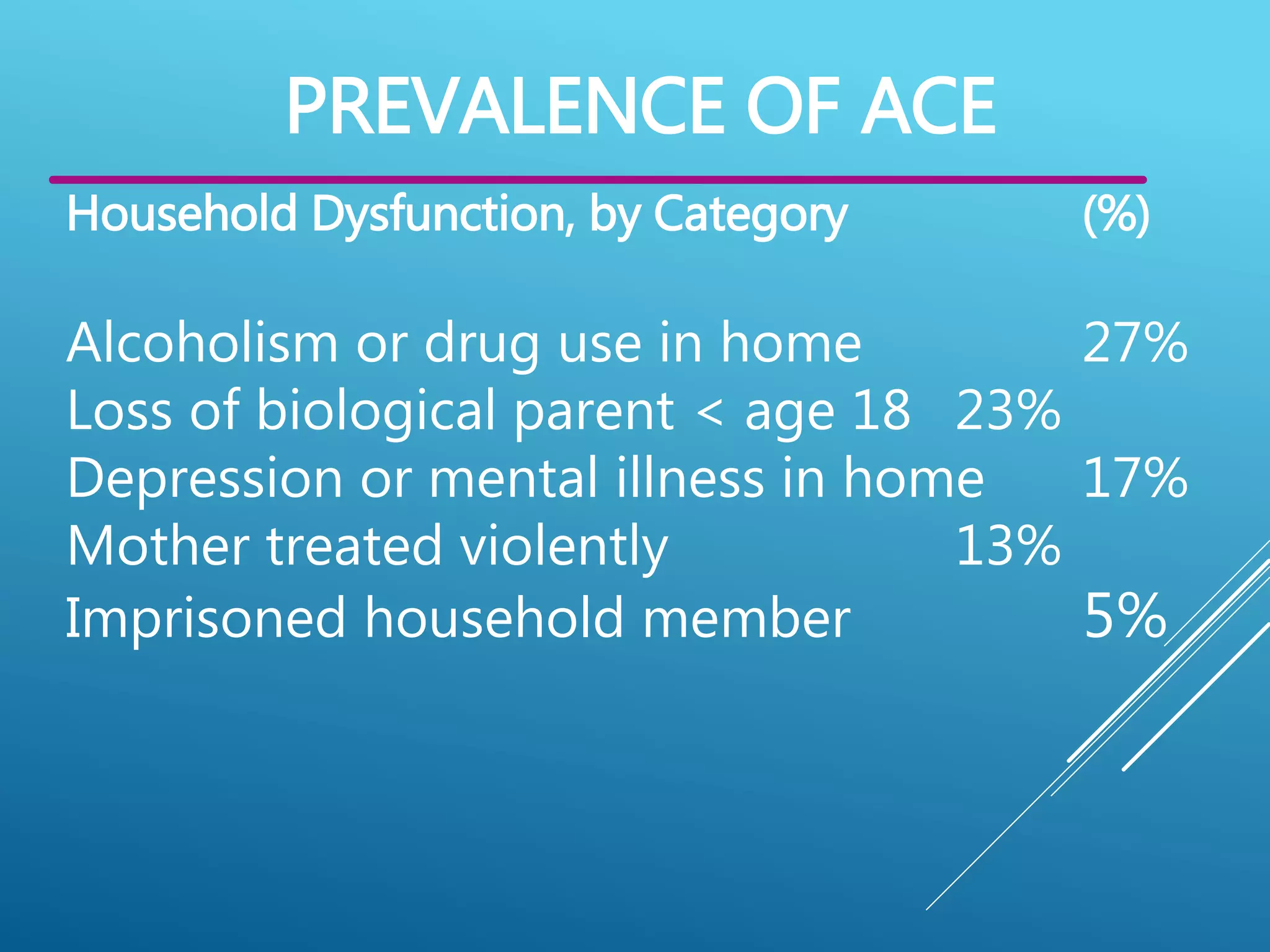
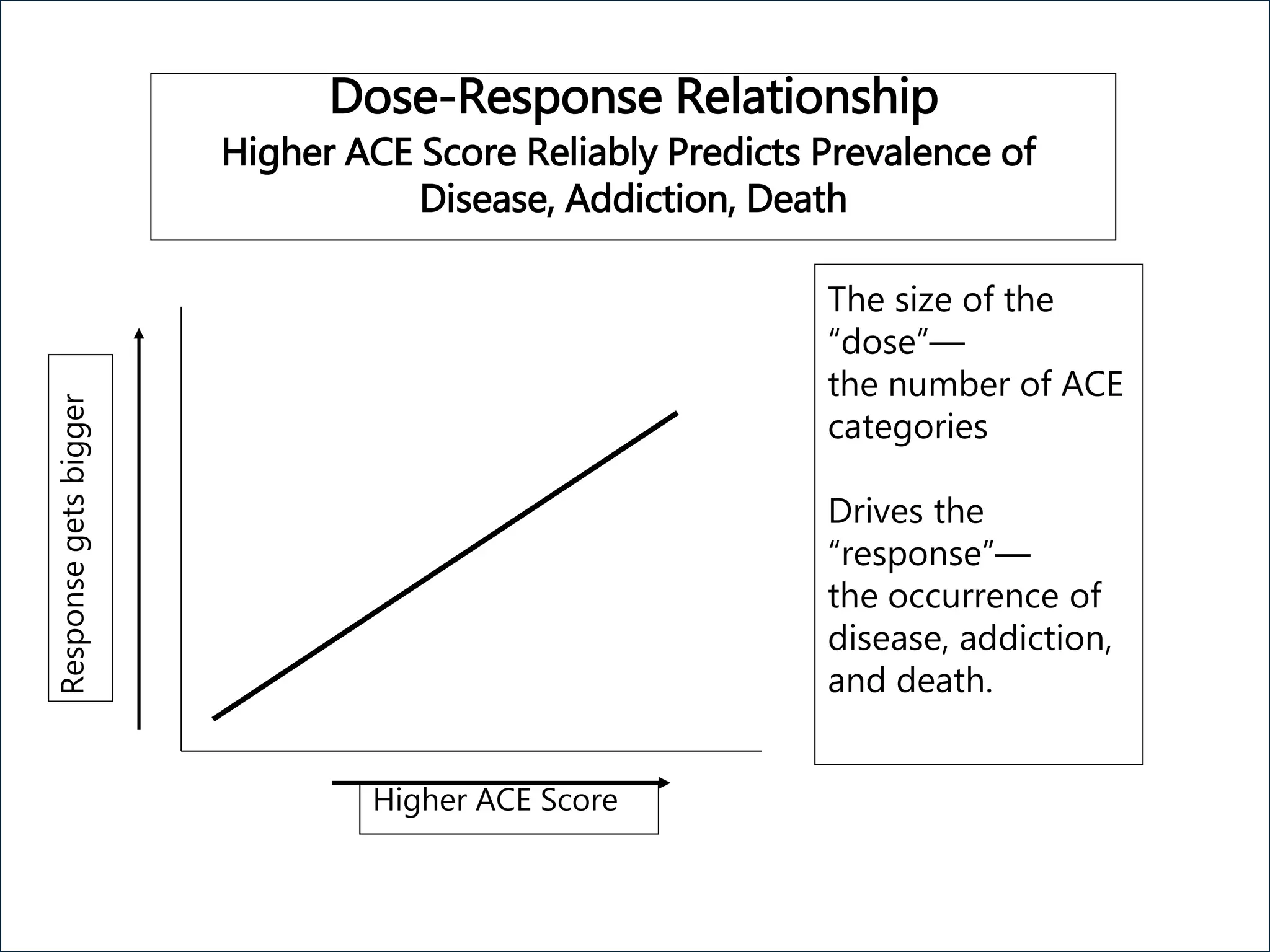
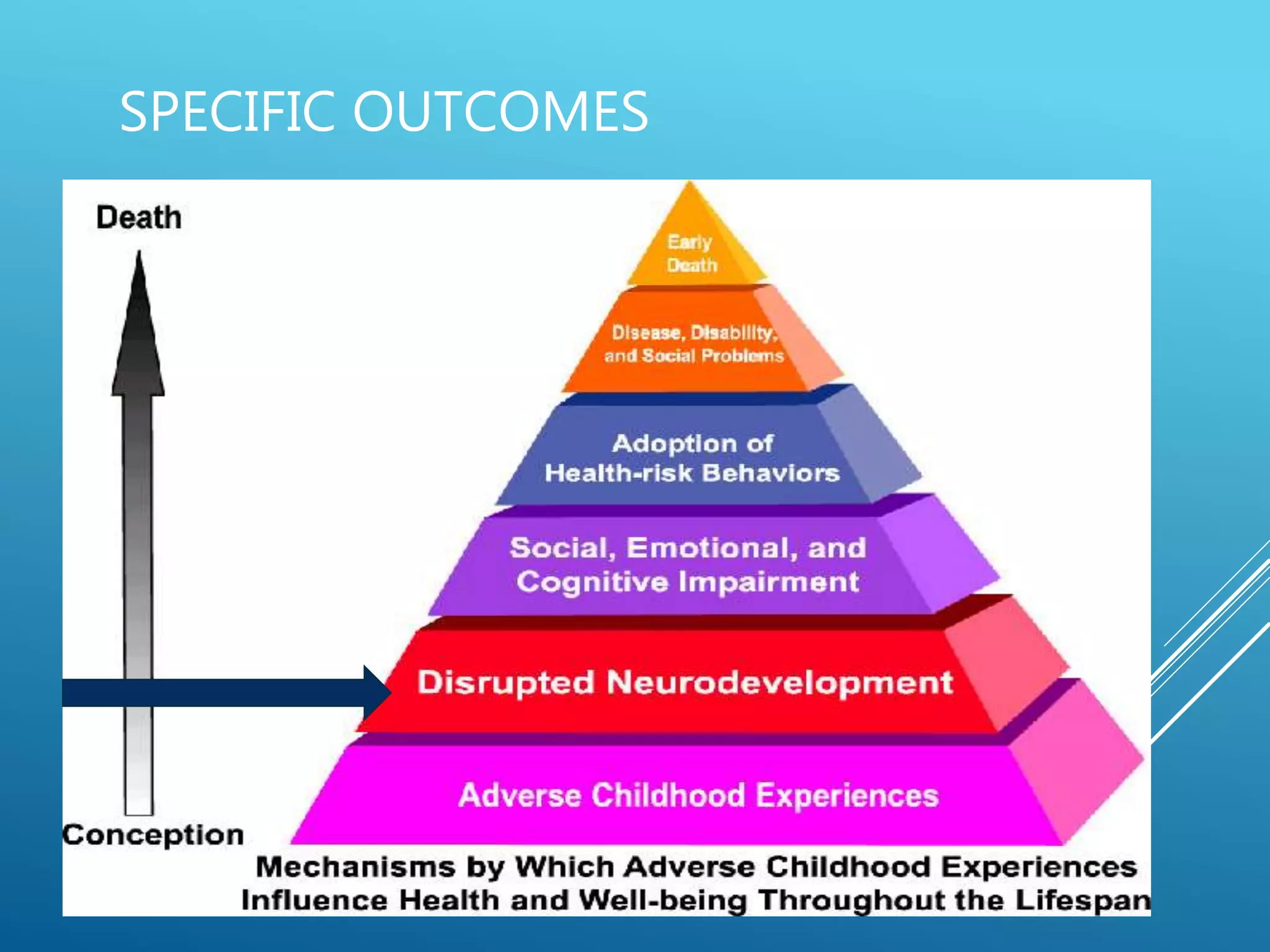
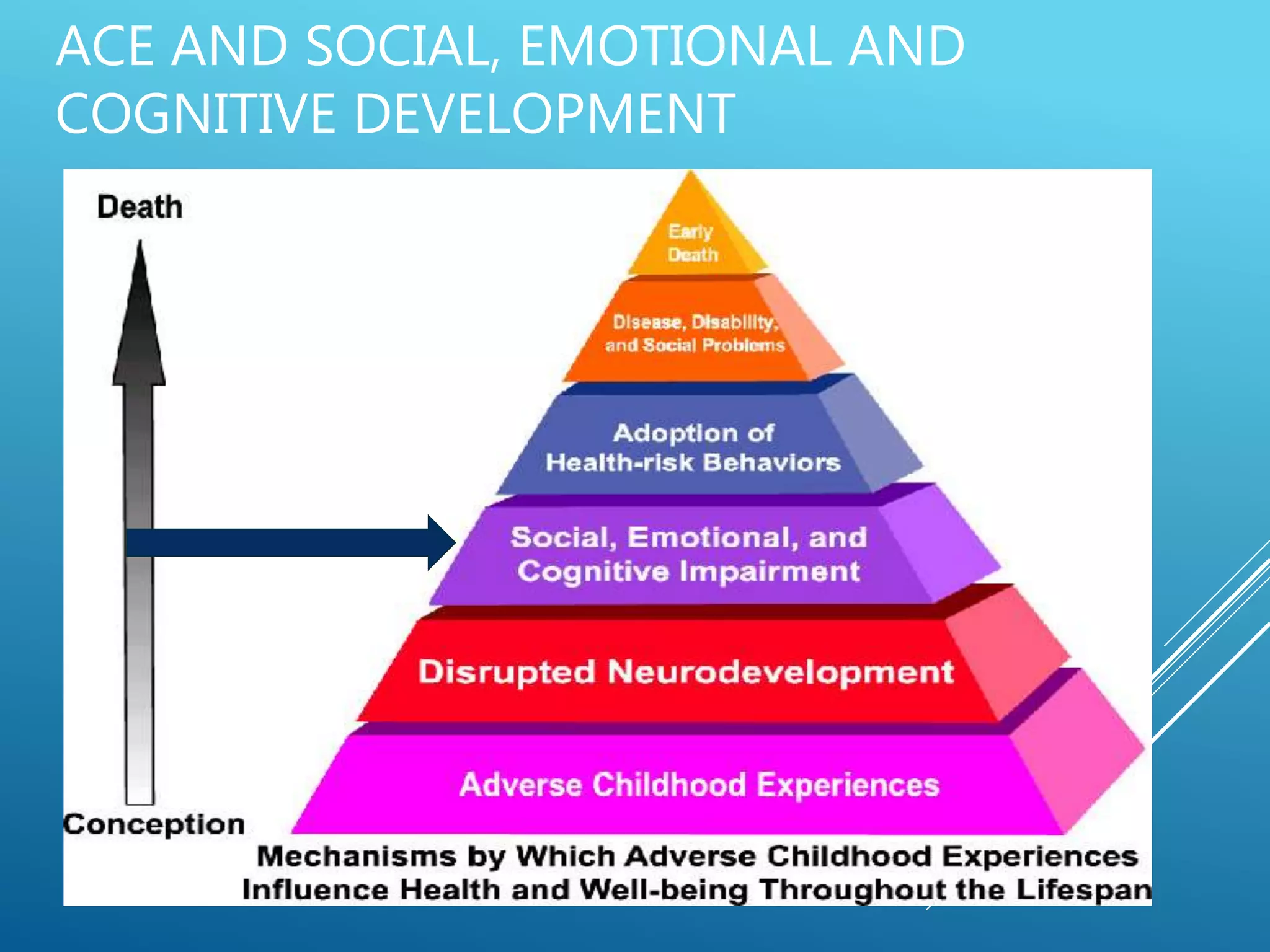
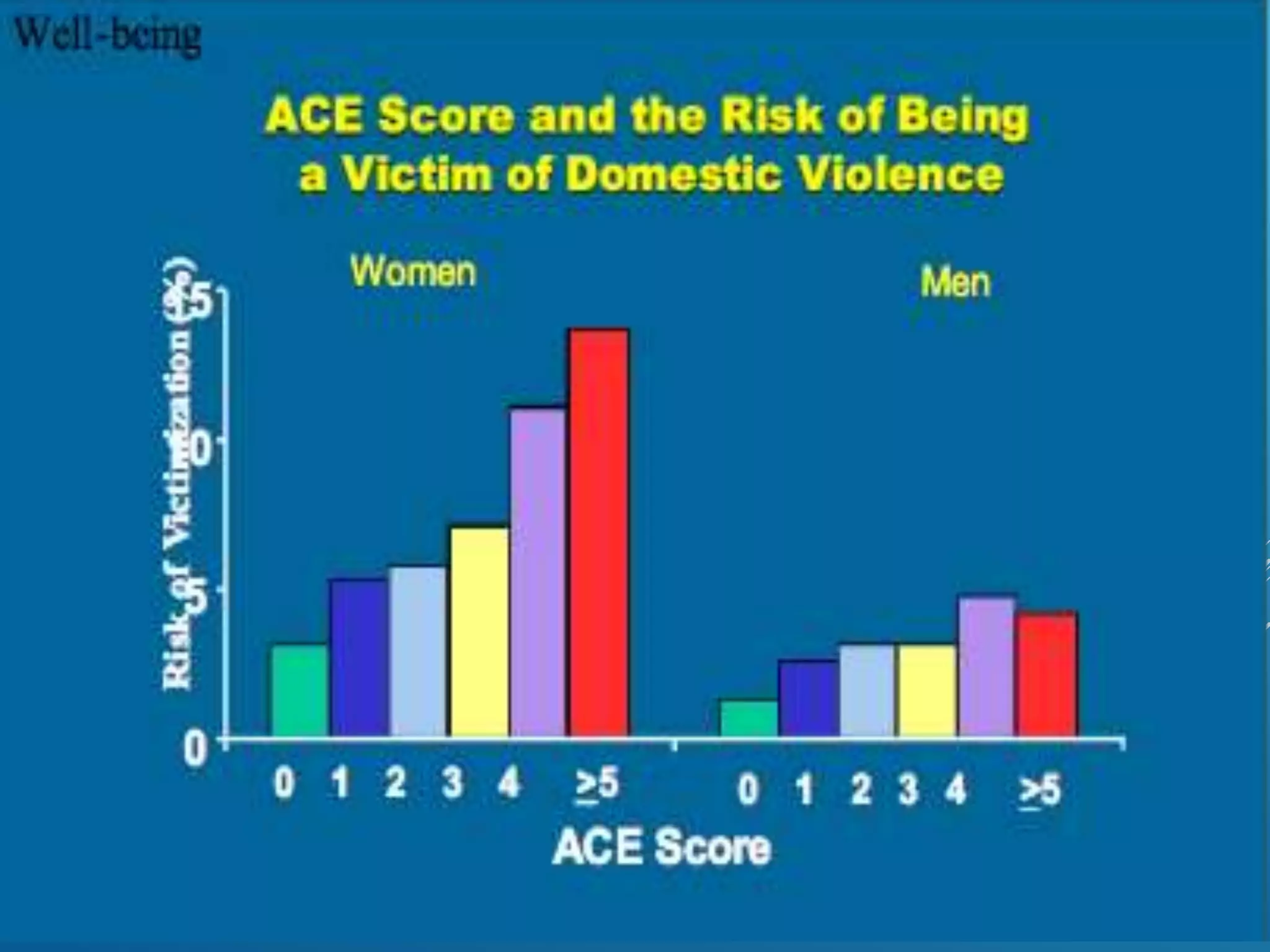
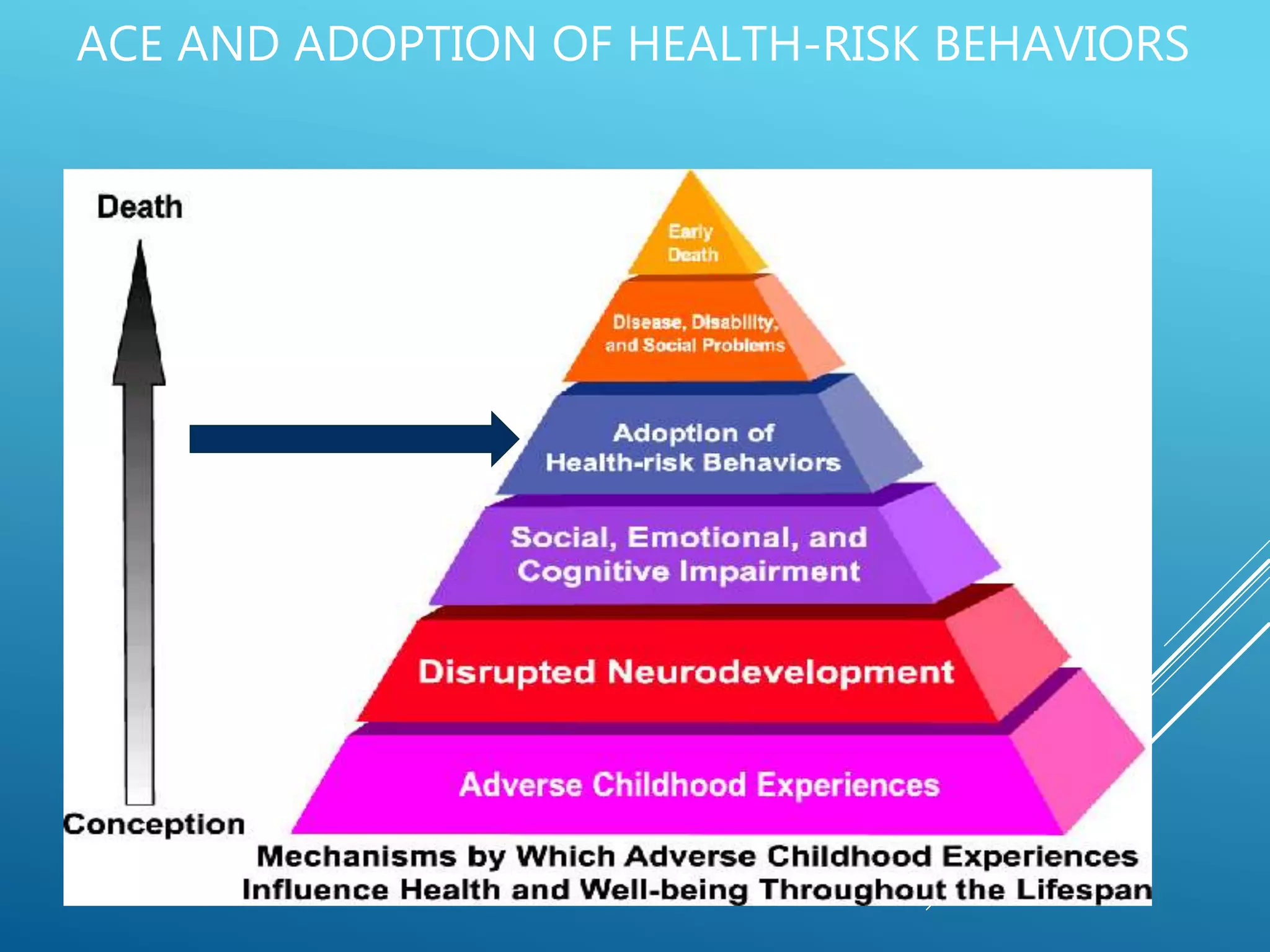
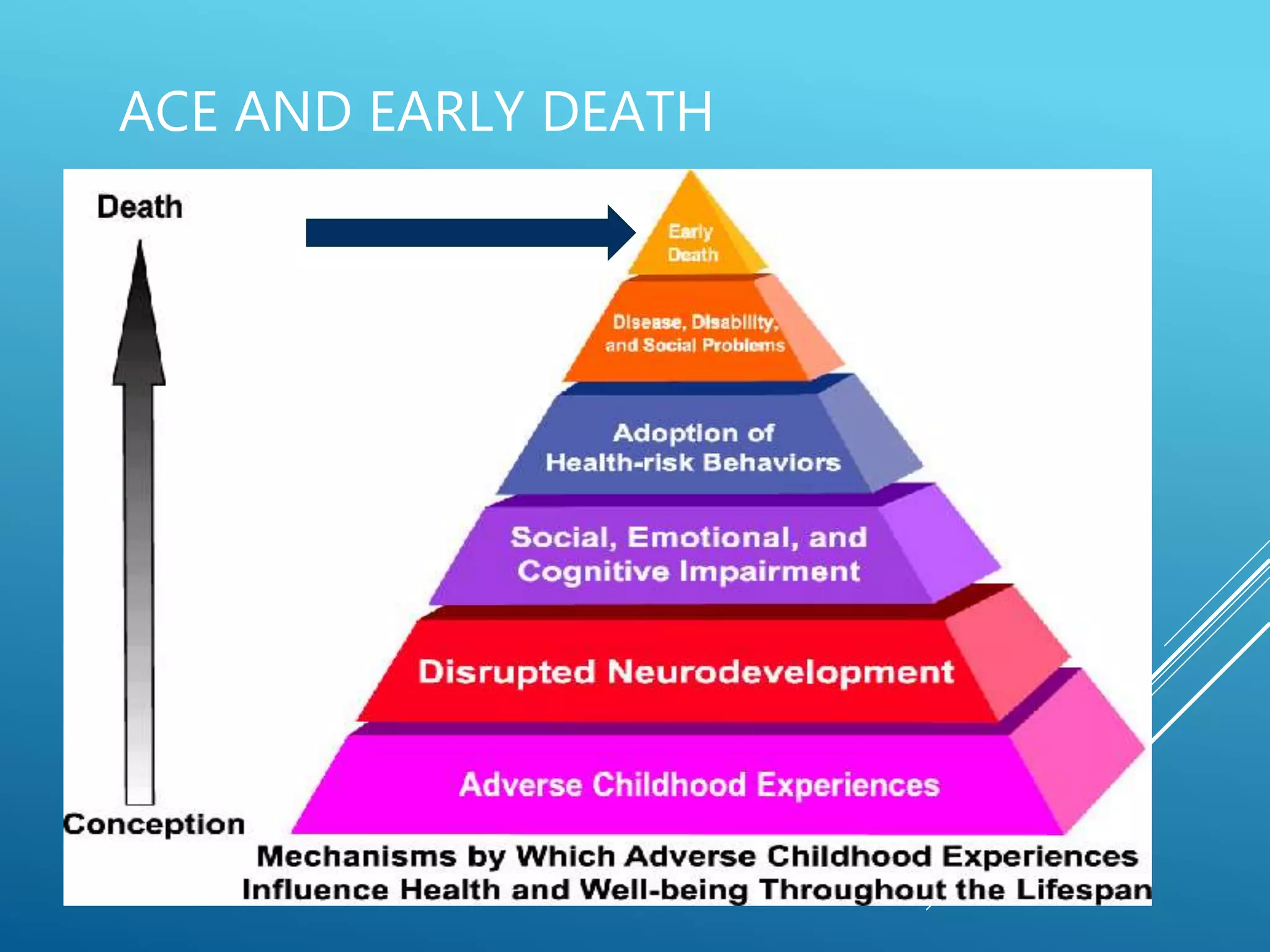
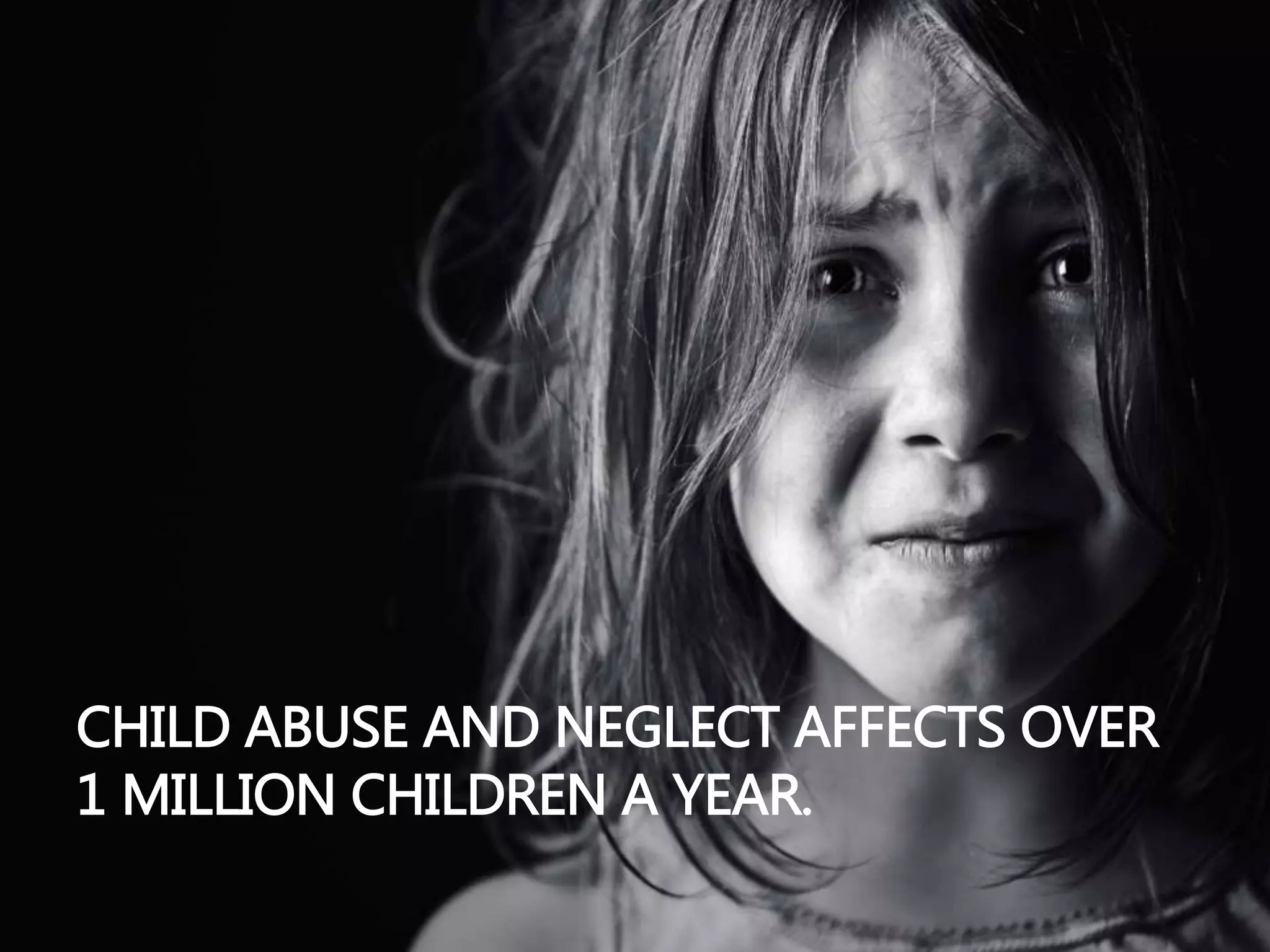
Dr. Denice Colson emphasizes that a significant portion of individuals in behavioral health settings have faced trauma, with 71% of self-reporting addicts indicating similar experiences. The document discusses the importance of understanding Adverse Childhood Experiences (ACEs) and their long-term effects on health and behavior, highlighting the relationship between trauma and various negative outcomes, including addiction, mental health issues, and reduced life expectancy. It advocates for trauma-informed care approaches in counseling, encouraging professionals to recognize and address trauma as a fundamental aspect of treatment.