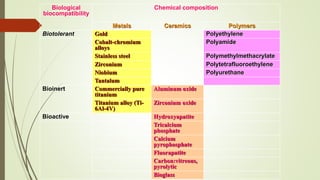
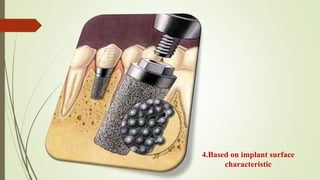
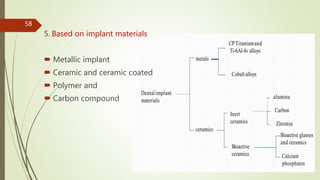
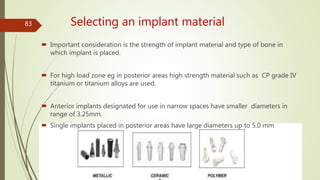
Implant materials can be classified based on their chemical composition, biological properties, design, surface characteristics, and type of material. Titanium and its alloys are the most commonly used metallic implant materials due to their excellent biocompatibility, corrosion resistance, and ability to osseointegrate. Other commonly used implant materials include cobalt-chromium alloys, stainless steel, ceramics, and polymers. Selecting the appropriate implant material depends on factors like the patient's health, bone quality, and intended use of the implant.