Downloaded 268 times
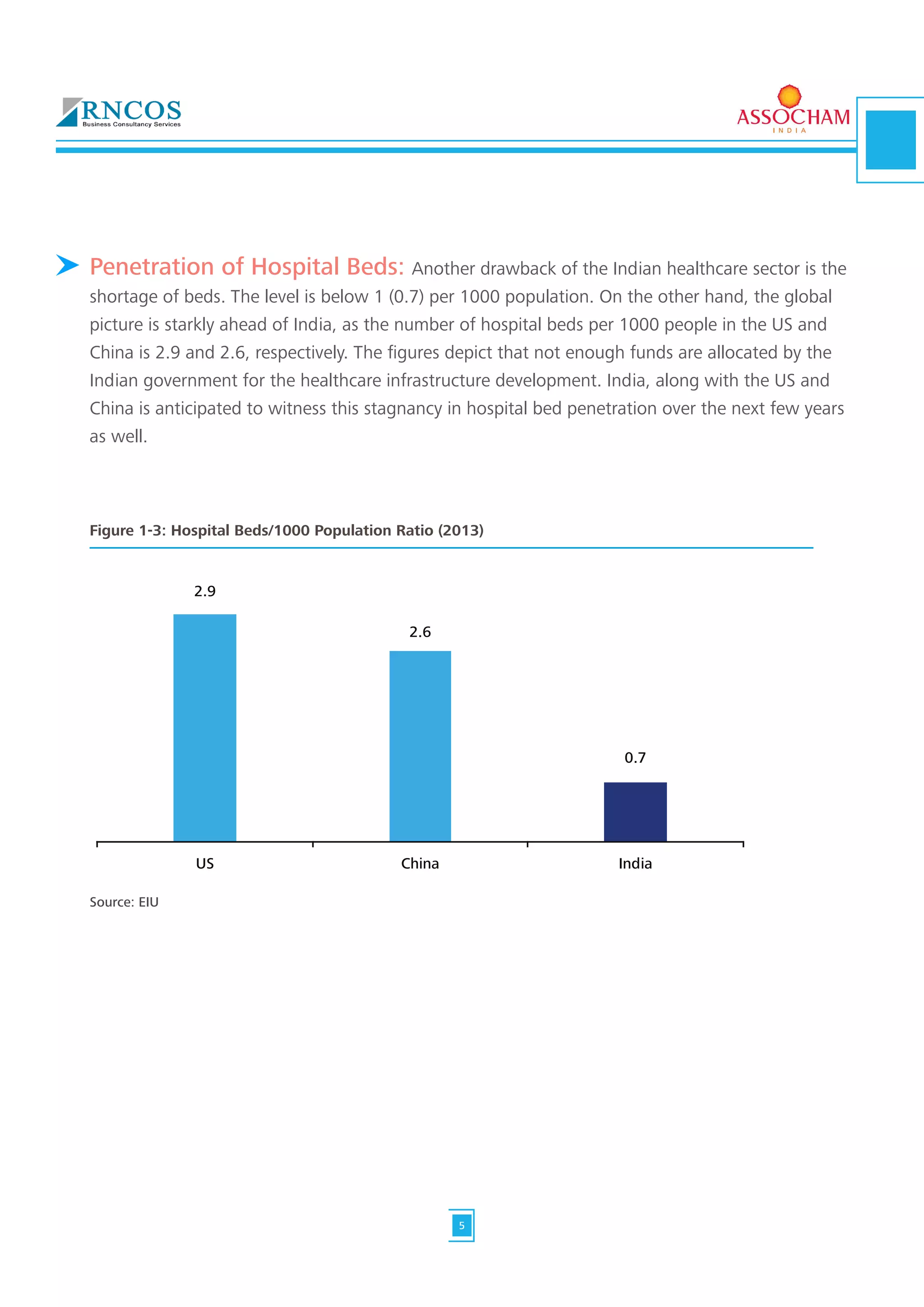
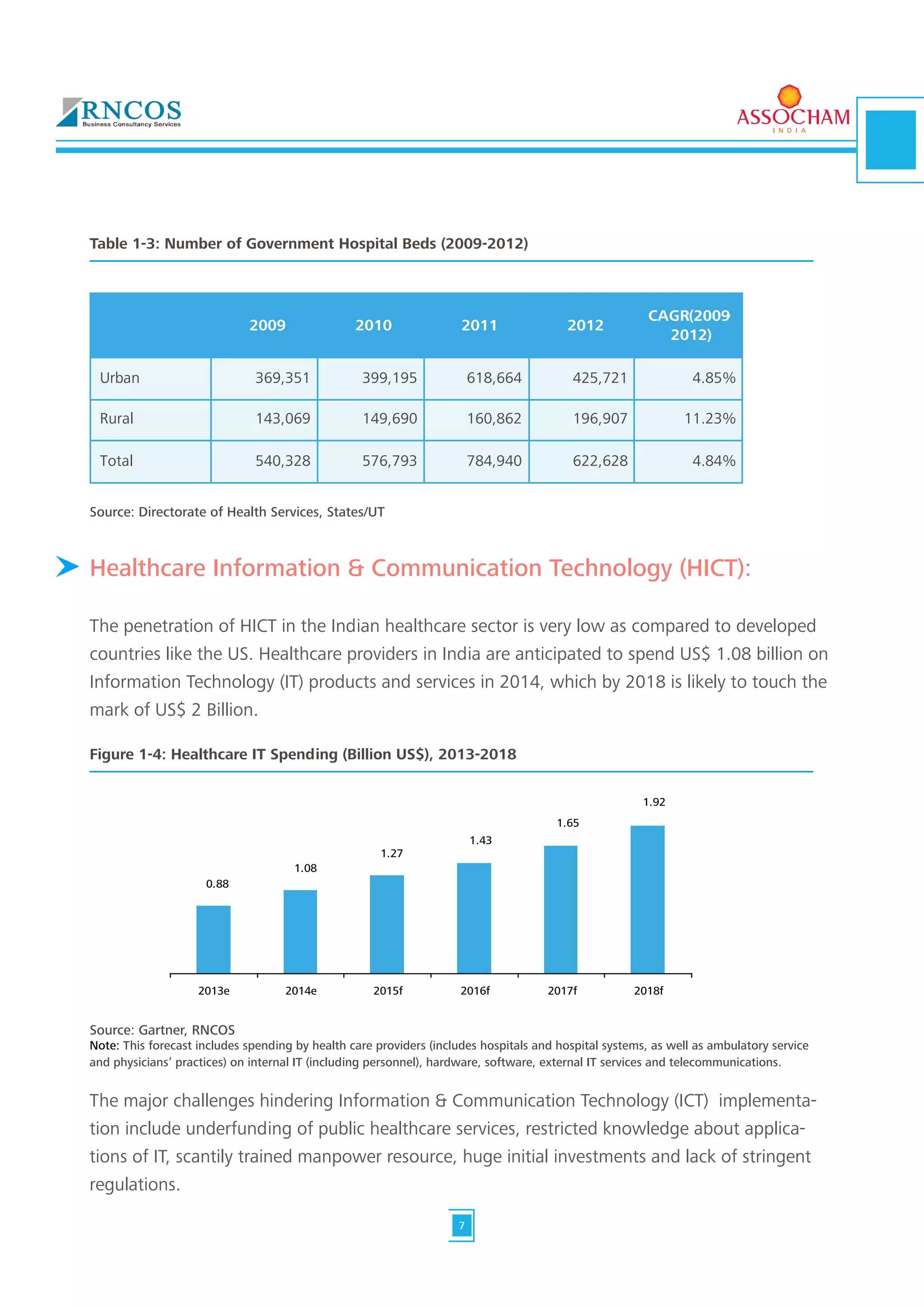


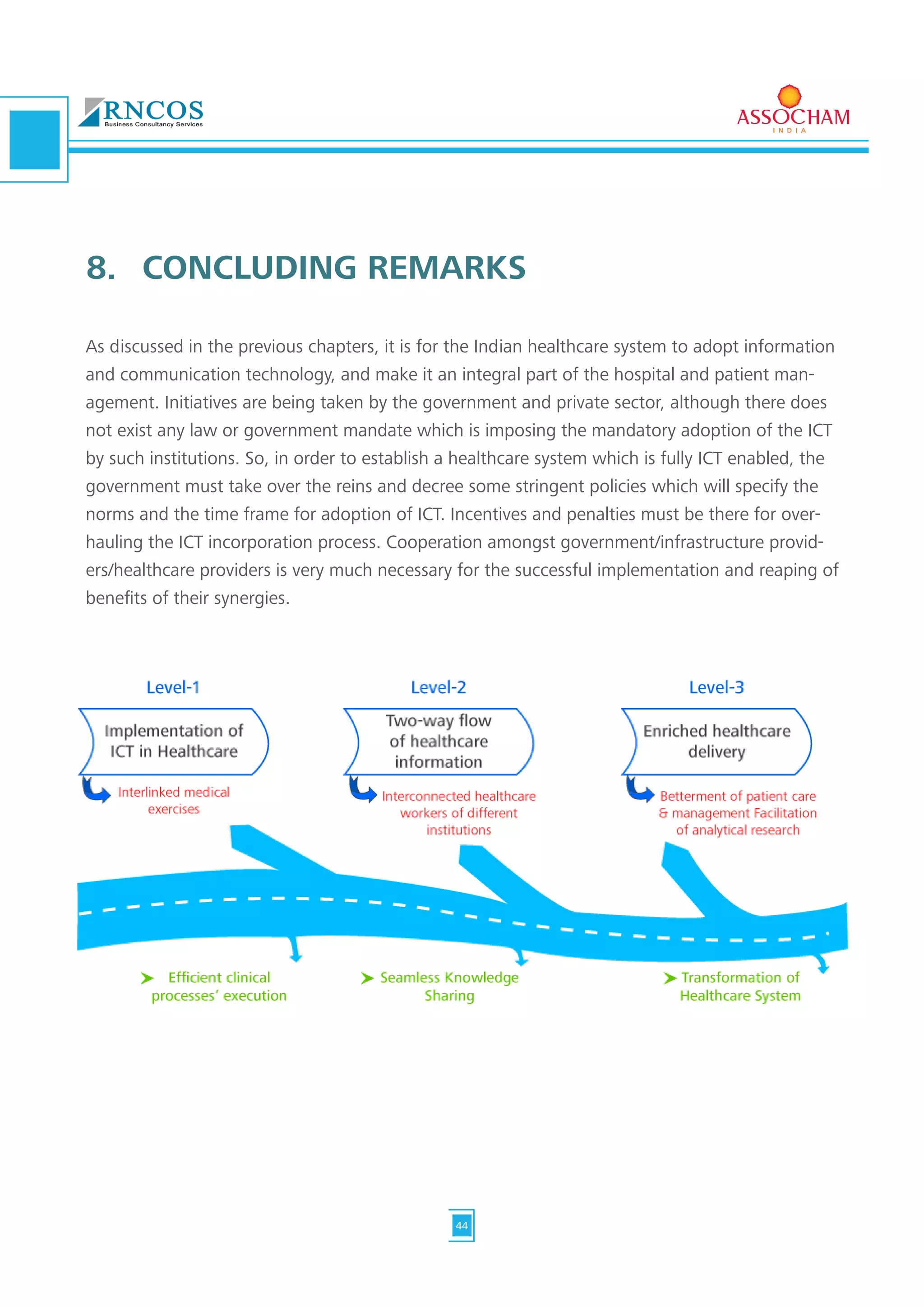

The document discusses challenges and opportunities for information and communication technology (ICT) in India's healthcare sector. It notes that while ICT could help address issues like the shortage of doctors and hospital beds in rural areas, the sector faces challenges like low government healthcare spending, lack of infrastructure, and lack of awareness and access in rural areas. The document advocates for government policies to better implement ICT and realize its potential to improve healthcare access, quality and lower costs.






















































































