This presentation provides an in-depth overview of Hypercapnic respiratory failure, including its pathophysiology, clinical aspects, causes and diagnostic approach and management strategies.
INTRODUCTION
• Occurrence
• canoccur in various settings, including emergency departments, inpatient units, postoperative
environments, and intensive care units.
• Underestimated Risk
• Acute hypercapnia is frequently overlooked, leading to delayed diagnosis and treatment.
• Potential Consequences
• If left untreated, may escalate to life-threatening conditions such as respiratory arrest, seizures,
coma, and ultimately, death.
3.
TYPES OF RESPIRATORYFAILURE
• Hypoxaemic (Type I) respiratory failure
• Unable to adequately provide Oxygen
• Partial pressure of oxygen (PaO2) < 60 mmHg
• Normal or decreased partial pressure of carbon dioxide (PaCO2)
• Alveolar-arterial (A-a) gradient Normal or Increased (depending on cause)
• Hypercapnic (Type II) respiratory failure
• Unable to sufficiently remove CO2
• Increase in arterial carbon dioxide (PaCO2)> 45 mmHg with a pH < 7.35
• Respiratory pump failure and/or Increased CO2 production
4.
M E CH AN I S M & E T I O LO GY
• Hypercapnia
• elevation in the arterial CO2 tension (PaCO2)
• Arterial CO2 directly proportional to production
inversely proportional to alveolar ventilation
• VA =VE x [1 -VD/VT]
• Dead space Minute ventilation – common causes
A – alveolar ventilation
E – minute ventilation
D – dead space
T – tidal volume
5.
PAT H OP H YS I O L O G Y
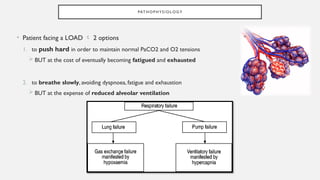
• Patient facing a LOAD 2 options
1. to push hard in order to maintain normal PaCO2 and O2 tensions
BUT at the cost of eventually becoming fatigued and exhausted
2. to breathe slowly, avoiding dyspnoea, fatigue and exhaustion
BUT at the expense of reduced alveolar ventilation
6.
V E NT I L ATO RY P U M P FA I L U R E
• 3 major causes
Inadequate
output from
respiratory centre
• Anaesthesia
• Drug overdose
• Disease of Medulla
Defects of
respiratory
muscles
• GBS
• Polio
• myopathies
Working under
excessive
inspiratory load
• Dynamic
hyperinflation
• Severe ILD
7.
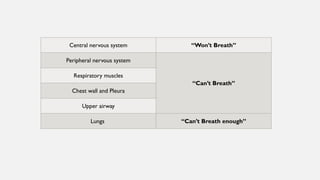
Central nervous system“Won’t Breath”
Peripheral nervous system
“Can’t Breath”
Respiratory muscles
Chest wall and Pleura
Upper airway
Lungs “Can’t Breath enough”
8.
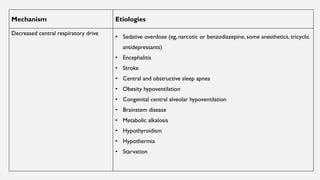
Mechanism Etiologies
Decreased centralrespiratory drive
• Sedative overdose (eg, narcotic or benzodiazepine, some anesthetics, tricyclic
antidepressants)
• Encephalitis
• Stroke
• Central and obstructive sleep apnea
• Obesity hypoventilation
• Congenital central alveolar hypoventilation
• Brainstem disease
• Metabolic alkalosis
• Hypothyroidism
• Hypothermia
• Starvation
Anatomical • Shortshallow breathing
Physiological • Pulmonary embolism (usually severe)
• Pulmonary vascular disease (usually severe)
• Dynamic hyperinflation (eg, upper and lower airway disorders including COPD,
severe asthma)
• End-stage interstitial lung disease
Increased CO2 production • Fever
• Thyrotoxicosis
• Increased catabolism (sepsis, steroids)
• Overfeeding
• Metabolic acidosis
• Exercise
Multifactorial • Severe laryngeal or tracheal disorders
(stenosis/tumors/angioedema/tracheomalacia)
• Vocal cord paralysis
• Epiglottitis upper airway disorders
• Foreign body aspiration
• Retropharyngeal disorders
• Obstructive goiter
12.
CLINICAL PRESENTATION
• Whento suspect Acute Hypercapnia….?
At risk of Hypoventilation sedative use, history of sleep apnea…
Increased dead space and limited pulmonary reserve COPD
SOB
Altered mental status
New hypoxemia
Hypersomnolence
Mild to moderate OR
Slowly developing Hypercapnia
Anxiety, Mild dyspnea, Daytime sluggishness, Headache,
Hypersomnolence
Higher levels of CO2 OR
Rapidly developing Hypercapnia
Delirium, Paranoia, Depression, Confusion, Coma
(CO2 narcosis)
Severe Hypercapnia Asterixis, Myoclonus, Seizures, Papilledema, Dilated superficial
veins
13.
D I AGN O S T I C E VA L UAT I O N
• History
• Risk factors:- sedative use…
• Chronic lung disease:- Bronchiectasis, Cystic fibrosis,Thoracic cage abnormalities…
• Obvious neuromuscular disorders:- hemiplegia, obesity, snoring…
• Patients on oxygen recent changes in the flow settings
• Post-operative / post-anaesthetic period hypoventilation
• Commonly missed
• Tendency to treat hypoxemia with O2 may worsen hypercapnia
I N VE S T I G AT I O N S
• Serum chemistries, bicarbonate, and electrolytes
• Raised HCO3 – may suggest underlying Chronic hypercapnia
• Hypomagnesemia and Hypophosphatemia – may suggest hypercapnia
• FBC – Polycythemia
• Toxicology screen - Opiates, Benzodiazepines, Tricyclic antidepressants, Barbiturates
• CPK – elevated CPK may suggest,
• Infectious or autoimmune polymyositis
• Hypothyroidism
• Rhabdomyolysis secondary to Colchicine or Chloroquine toxicity
• Procainamide myopathy
16.
• Imaging assessment
•CXR should be performed – intrapulmonary pathology
• COPD – hyperinflation, flattened diaphragm
• ILD – reticular nodular shadows
• Thoracic cage - kyphoscoliosis, pectus excavatum, ankylosing spondylitis, fractured ribs, diaphragmatic paralysis
• Brain and Spinal cord imaging
• Stroke,Tumor,Traumatic transection of the spinal cord
• Physiologic assessment
• Serial bedsideVC measurements – helpful in pts with Myasthenic crisis
• VC <1 L in a patient with normal baseline lung function increased risk of RF
• Previous sleep studies, NCS or EMG underlying sleep apnea or neuromyopathy
17.
• Arterial BloodGas (ABG)
• Arterial CO2 tension [PaCO2] >45 mmHg – diagnostic of Hypercapnia
• ACUTE
• always accompanied by Respiratory Acidosis (pH < 7.35)
• In pure acute respiratory acidosis with previous normocapnia measured level of hypercapnia and bicarbonate accurately
predicts the pH
• Acute-on-Chronic respiratory acidosis measured pH will be higher than predicted
• CHRONIC
• low-normal or near-normal pH
• Raised HCO3 indicative of renal compensation
18.
• Alveolar-arterial gradient(PAO2 – PaO2) (A-a gradient)
• Calculated from a room air ABG
• Can distinguish Global Hypoventilation from Abnormal gas exchange
• In global hypoventilation Normal A-a gradient (<20mmHg) with elevated PCO2
• In underlying lung disease Widened A-a gradient
19.
M A NAG E M E N T
• ABC approach
• AIRWAY – upper airway obstruction
• OXYGEN
• For clinically significant desaturation (< 90%)
• Major concern – worsening hypercapnia and acidosis
• Efforts to lower PaCO2 improve oxygenation
• Oxygen targets
• In general SPO2 90% - 93% (PaO2 of 60 to 70 mmHg)
• **Patients with severe chronic hypoxic hypercapnic respiratory failure, levels lower than that (≥88% or PaO2 >55 to 60 mmHg)
may be maintained especially if it is close to their baseline and the patient is clinically stable (eg, normal mentation).
• Adequate treatment of
Hypoxemia
Primary goal
• Avoidance of worsening
hypercapnia
Secondary
goal
20.
• Initial OxygenLevels:
• Begin with low flow: 1 to 2 L/min or 24 to 28% FiO2.
• Goal:Achieve SpO2 at or near target.
• Incremental Increases:
• Nasal cannula: Increase by 1 L/min.
• Venturi mask: Increase by 4 to 7%.
• Monitoring:
• Monitor PaO2 and PaCO2 closely during increments.
• Maintenance andWeaning:
• Maintain achieved SpO2 level.
• Gradual weaning as underlying issues resolve.
21.
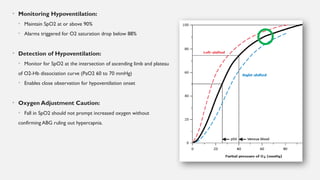
• Monitoring Hypoventilation:
•Maintain SpO2 at or above 90%
• Alarms triggered for O2 saturation drop below 88%
• Detection of Hypoventilation:
• Monitor for SpO2 at the intersection of ascending limb and plateau
of O2-Hb dissociation curve (PaO2 60 to 70 mmHg)
• Enables close observation for hypoventilation onset
• Oxygen Adjustment Caution:
• Fall in SpO2 should not prompt increased oxygen without
confirming ABG ruling out hypercapnia.
22.
• ApproachTolerance:
• Prolongedsevere hypoxemia not tolerated.
• Titrating oxygen suitable for quick responders or those without complications. (chest pain, altered mental status, lactic acidosis)
• Severe Hypoxemia (SpO2 65%)
• Administer oxygen for SpO2 90 to 93%.
• Worsening hypercapnia may require noninvasive or invasive ventilation.
• Respiratory Acidosis and Impaired Consciousness:
• Severe cases (pH <7.2, marked consciousness depression): Intubation and mechanical ventilation.
• Lesser acidosis and mild symptoms: Consider noninvasive ventilation and FiO2 reduction.
• Bicarbonate Ineffectiveness:
• Bicarbonate ineffective for acute respiratory acidosis.
• Address severe respiratory acidosis by increasing ventilation, not sodium bicarbonate.
23.
Suspected Oxygen-Induced HypercapnicRespiratory Failure:
• Oxygen saturation in high normal range (>95%).
• Lower supplemental oxygen to achieve 90-93% during arterial blood gases drawing.
Clinical Example: Obstructive Sleep Apnea:
• Postoperative desaturation in obstructive sleep apnea.
• 100% oxygen may improve oxygenation but worsen hypercapnia.
• Reduction in supplemental oxygen, with or without noninvasive ventilation, can avoid mechanical
ventilation.
Caution During Oxygen Reduction:
• Avoid marked hypoxemia during FiO2 reduction.
• Risk of both hypercapnia and hypoxemia, potentially requiring intubation.
24.
Oxygen-Induced Hypercapnic RespiratoryFailure with Low Normal Saturation:
• Saturation in low normal range (88-93%) in chronic hypoxic hypercapnic respiratory
failure.
• Options:
• Fine titration of supplemental oxygen.
• Noninvasive ventilation.
• Mechanical ventilation.
Cautionary Note:
• Do not entirely remove oxygen to avert intubation.
• Complete removal of O2 may worsen tissue hypoxemia and acidosis.
25.
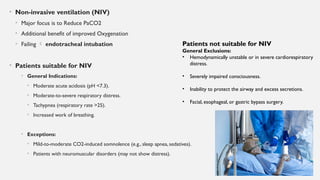
• Non-invasive ventilation(NIV)
• Major focus is to Reduce PaCO2
• Additional benefit of improved Oxygenation
• Failing endotracheal intubation
• Patients suitable for NIV
• General Indications:
• Moderate acute acidosis (pH <7.3).
• Moderate-to-severe respiratory distress.
• Tachypnea (respiratory rate >25).
• Increased work of breathing.
• Exceptions:
• Mild-to-moderate CO2-induced somnolence (e.g., sleep apnea, sedatives).
• Patients with neuromuscular disorders (may not show distress).
Patients not suitable for NIV
General Exclusions:
• Hemodynamically unstable or in severe cardiorespiratory
distress.
• Severely impaired consciousness.
• Inability to protect the airway and excess secretions.
• Facial, esophageal, or gastric bypass surgery.
26.
• Mode –While most patients are started on pressure-controlled NIV [BiPAP] some patients may demonstrate improved
tolerance on volume-controlled NIV (eg, patients with neuromuscular disease)
• Mask – An oronasal mask is often chosen initially rather than full-face mask, a nasal mask, or nasal prongs
• Settings –The optimal initial settings vary depending upon the mode of NIV chosen. Most clinicians opt for lower
settings and titrate up depending upon the patient's ability to tolerate it and their response.
• Examples of initial settings for bedside NIV include:
• BiPAP – 8 to 12 cm H2O (inspiratory pressure) and 3 to 5cm H2O (expiratory pressure).
• Pressure support NIV (PSV-NIV) – 8 to 12cm H2O (pressure support) and 3 to 5 cm H2O (positive end expiratory pressure).
• Volume-controlled NIV – Tidal volume 6 to 8 mL/kg and 5cm H2O PEEP; rate 10 to 12 breaths/minute.
27.
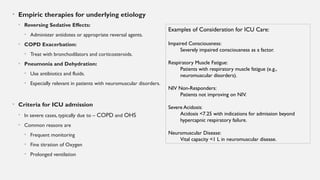
• Empiric therapiesfor underlying etiology
• Reversing Sedative Effects:
• Administer antidotes or appropriate reversal agents.
• COPD Exacerbation:
• Treat with bronchodilators and corticosteroids.
• Pneumonia and Dehydration:
• Use antibiotics and fluids.
• Especially relevant in patients with neuromuscular disorders.
• Criteria for ICU admission
• In severe cases, typically due to – COPD and OHS
• Common reasons are
• Frequent monitoring
• Fine titration of Oxygen
• Prolonged ventilation
Examples of Consideration for ICU Care:
Impaired Consciousness:
Severely impaired consciousness as a factor.
Respiratory Muscle Fatigue:
Patients with respiratory muscle fatigue (e.g.,
neuromuscular disorders).
NIV Non-Responders:
Patients not improving on NIV.
Severe Acidosis:
Acidosis <7.25 with indications for admission beyond
hypercapnic respiratory failure.
Neuromuscular Disease:
Vital capacity <1 L in neuromuscular disease.
#8 Hyperthyroidism also can rarely cause respiratory muscle weakness
#11 Upper airway disorders are rare causes of hypercapnia. They either diminish total ventilation or lead to dynamic hyperinflation and reduced tidal volume while simultaneously causing increased work of breathing and carbon dioxide production.
![M E C H AN I S M & E T I O LO GY
• Hypercapnia
• elevation in the arterial CO2 tension (PaCO2)
• Arterial CO2 directly proportional to production
inversely proportional to alveolar ventilation
• VA =VE x [1 -VD/VT]
• Dead space Minute ventilation – common causes
A – alveolar ventilation
E – minute ventilation
D – dead space
T – tidal volume](https://image.slidesharecdn.com/hypercapnicrespiratoryfailure-250419060244-1db23e1d/85/Hypercapnic-Type-2-respiratory-failure-pptx-4-320.jpg)


![• Arterial Blood Gas (ABG)
• Arterial CO2 tension [PaCO2] >45 mmHg – diagnostic of Hypercapnia
• ACUTE
• always accompanied by Respiratory Acidosis (pH < 7.35)
• In pure acute respiratory acidosis with previous normocapnia measured level of hypercapnia and bicarbonate accurately
predicts the pH
• Acute-on-Chronic respiratory acidosis measured pH will be higher than predicted
• CHRONIC
• low-normal or near-normal pH
• Raised HCO3 indicative of renal compensation](https://image.slidesharecdn.com/hypercapnicrespiratoryfailure-250419060244-1db23e1d/85/Hypercapnic-Type-2-respiratory-failure-pptx-17-320.jpg)

![• Mode – While most patients are started on pressure-controlled NIV [BiPAP] some patients may demonstrate improved
tolerance on volume-controlled NIV (eg, patients with neuromuscular disease)
• Mask – An oronasal mask is often chosen initially rather than full-face mask, a nasal mask, or nasal prongs
• Settings –The optimal initial settings vary depending upon the mode of NIV chosen. Most clinicians opt for lower
settings and titrate up depending upon the patient's ability to tolerate it and their response.
• Examples of initial settings for bedside NIV include:
• BiPAP – 8 to 12 cm H2O (inspiratory pressure) and 3 to 5cm H2O (expiratory pressure).
• Pressure support NIV (PSV-NIV) – 8 to 12cm H2O (pressure support) and 3 to 5 cm H2O (positive end expiratory pressure).
• Volume-controlled NIV – Tidal volume 6 to 8 mL/kg and 5cm H2O PEEP; rate 10 to 12 breaths/minute.](https://image.slidesharecdn.com/hypercapnicrespiratoryfailure-250419060244-1db23e1d/85/Hypercapnic-Type-2-respiratory-failure-pptx-26-320.jpg)






















![Acute_respiratory_failure[1] [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/acuterespiratoryfailure1autosaved-240613055024-837043a9-thumbnail.jpg?width=640&height=640&fit=bounds)

























