Downloaded 190 times

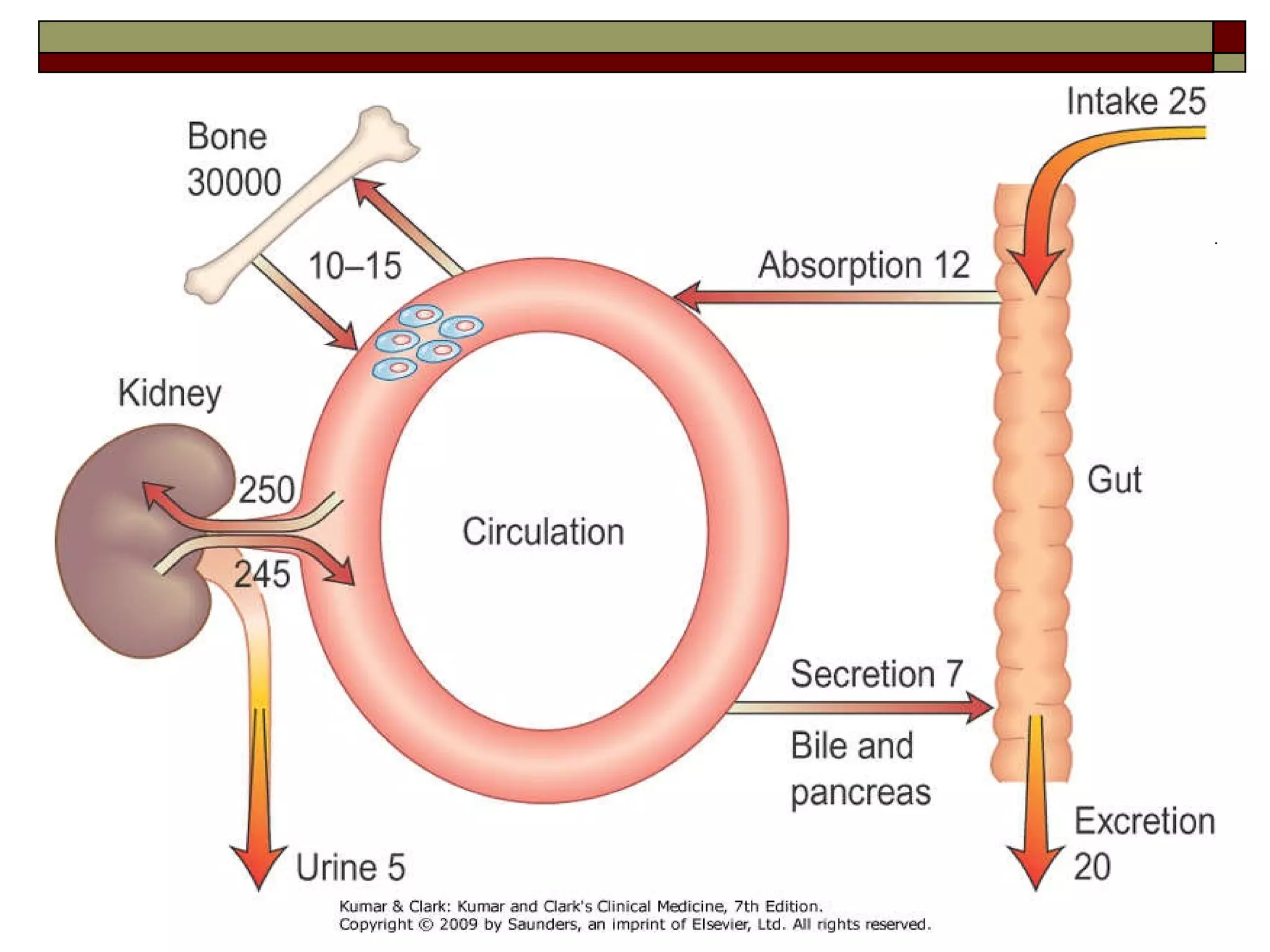
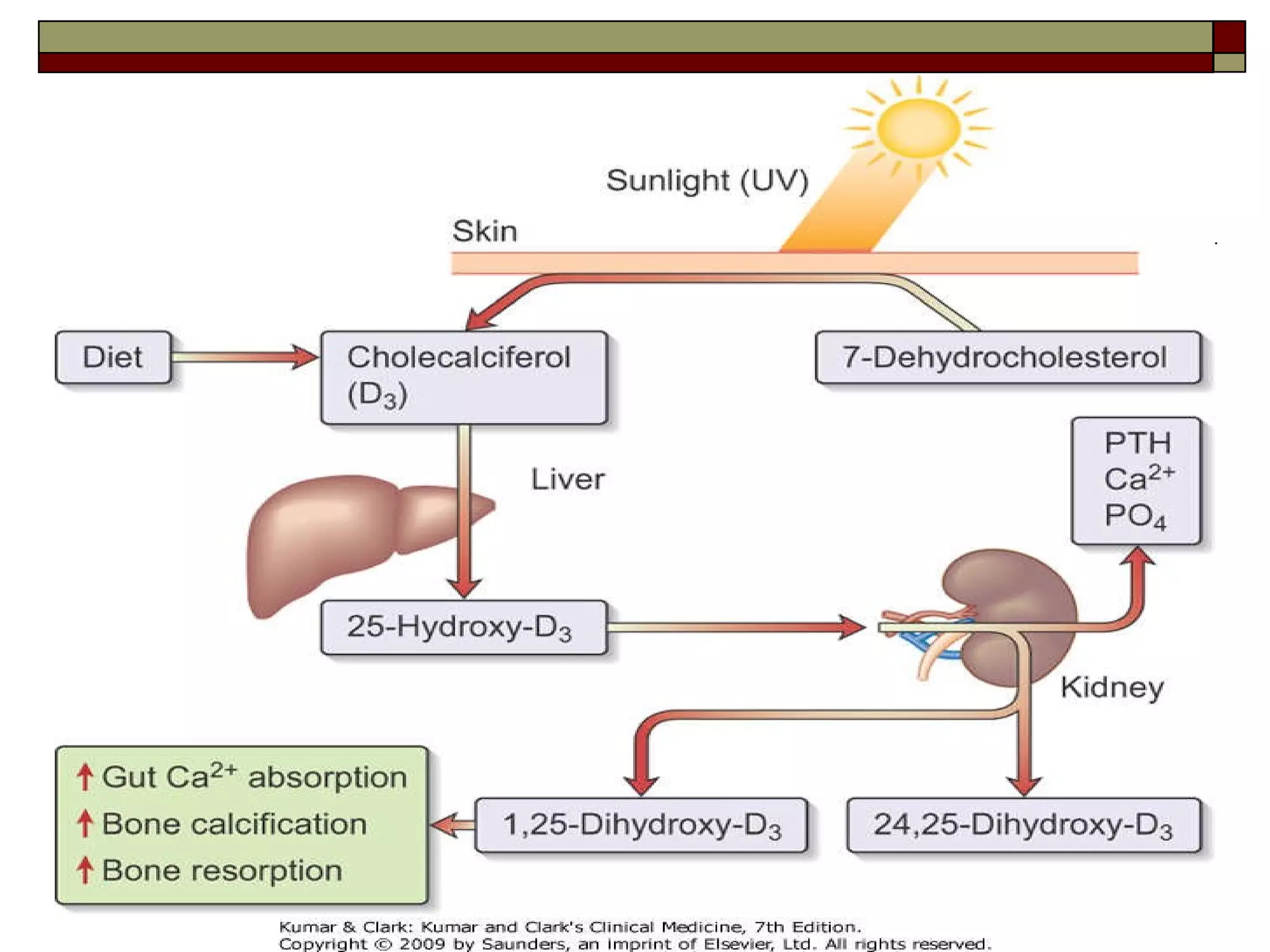
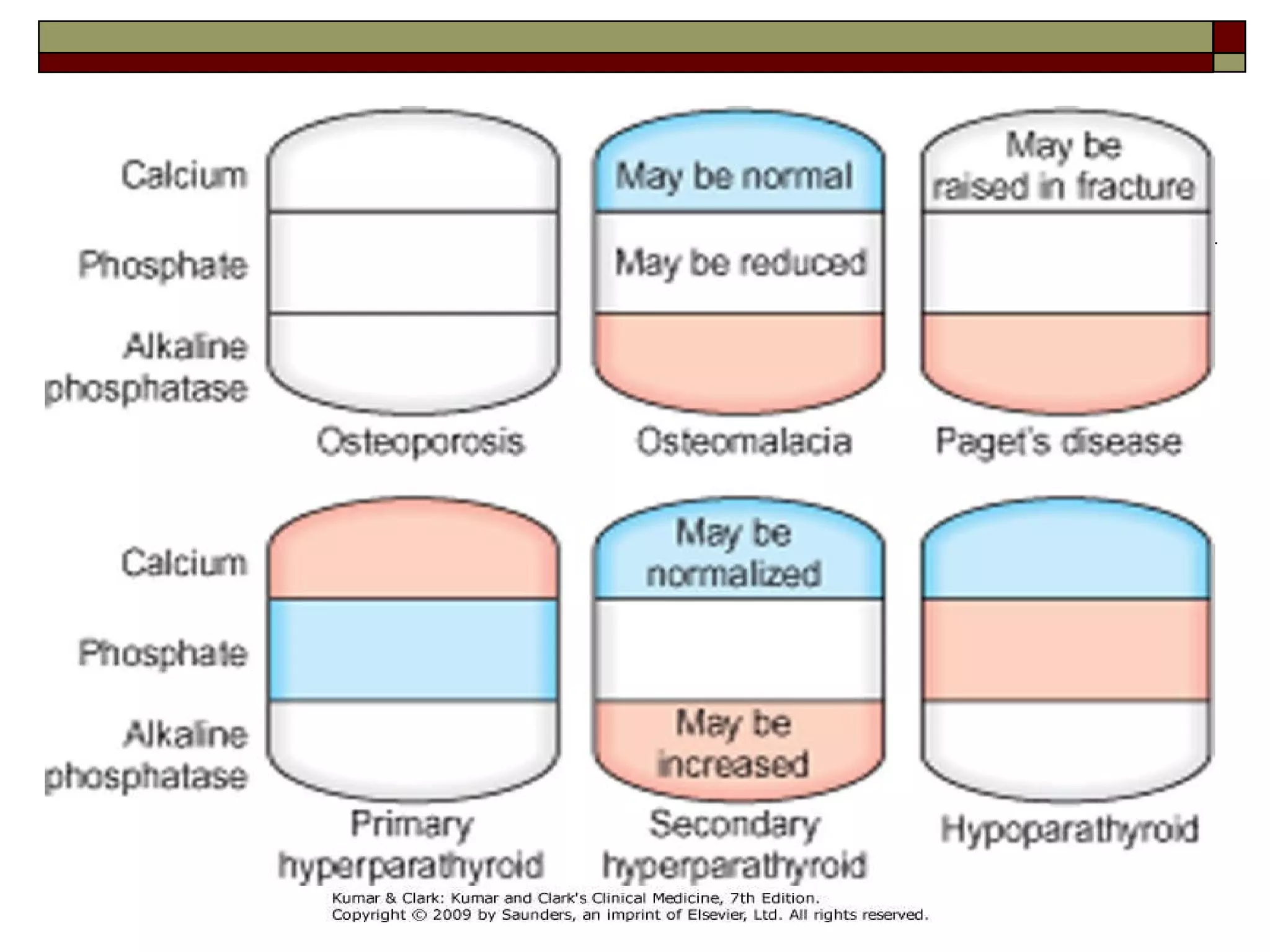
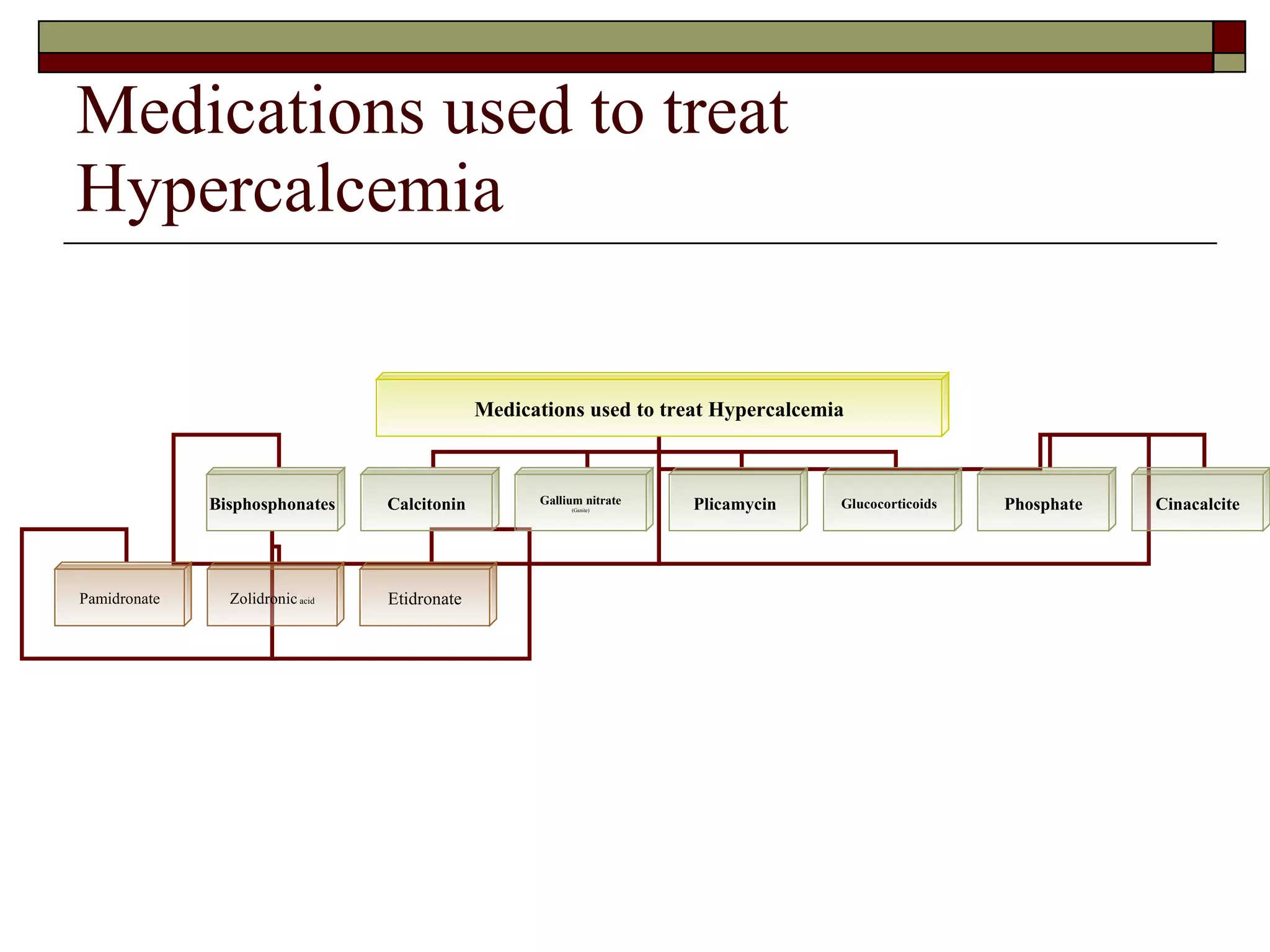


This document presents a case study of a 41-year-old woman diagnosed with hypercalcemia caused by milk alkali syndrome. She was brought to the emergency department with nausea, vomiting, and altered mental status. Tests found her blood calcium level to be very high. Her history of consuming large amounts of antacids containing calcium and sodium bicarbonate led to the diagnosis of milk alkali syndrome. Milk alkali syndrome occurs when excessive oral intake of calcium and alkali impairs the kidney's ability to excrete calcium, resulting in hypercalcemia. The document then provides background information on calcium regulation and the various causes, symptoms, diagnostic evaluation, and treatment approaches for hypercalcemia.







































































































