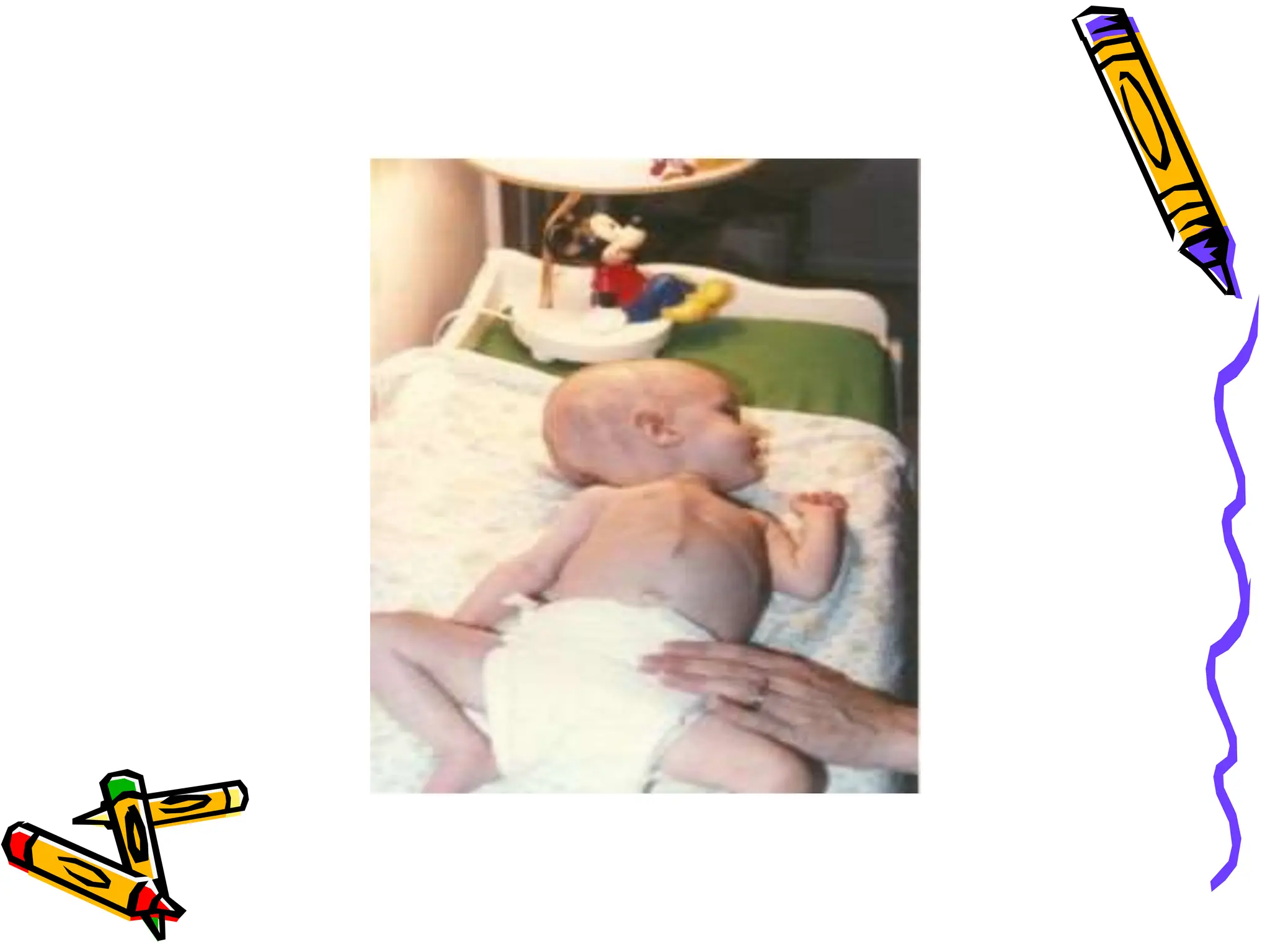
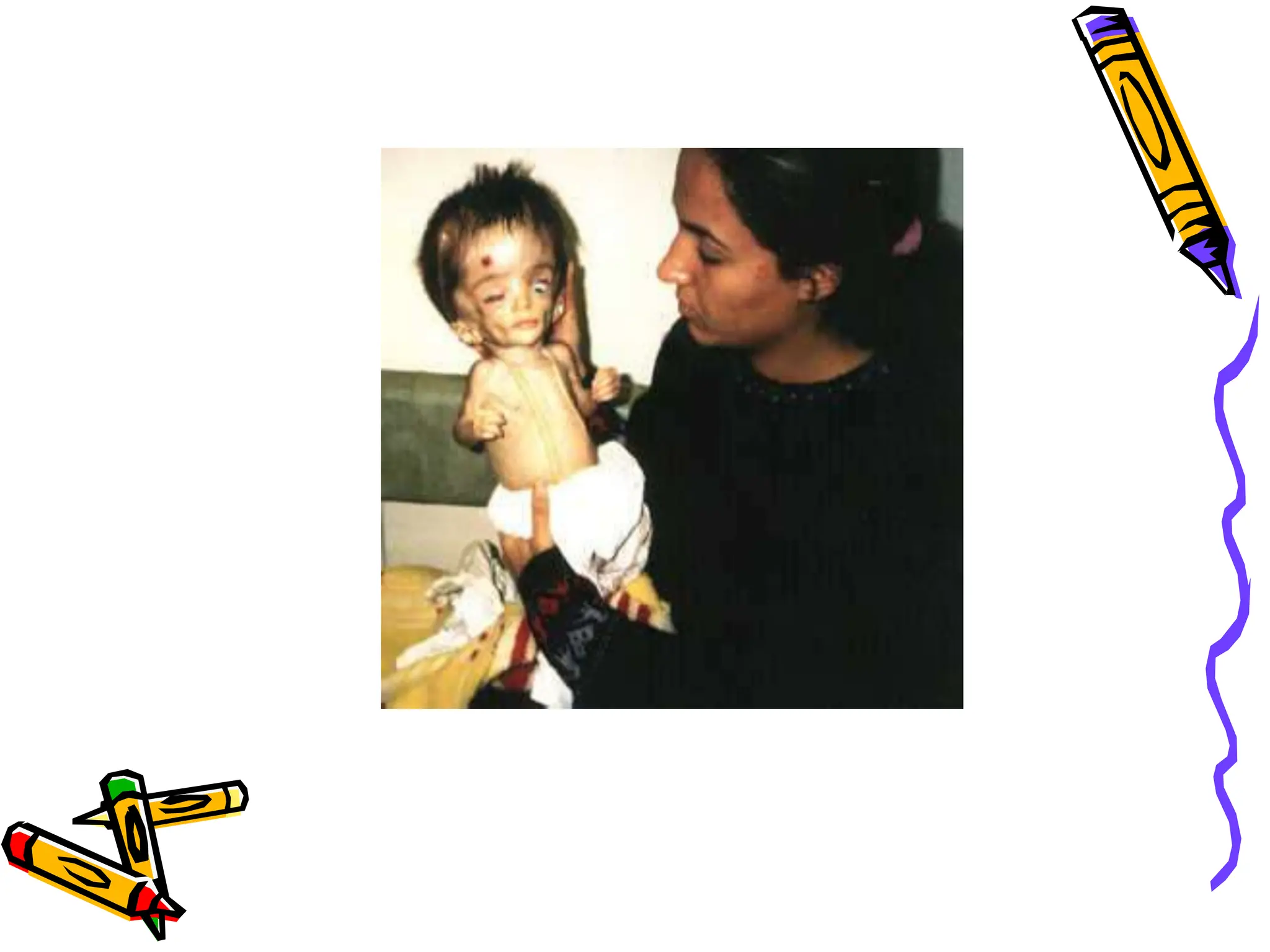
This document discusses hydrocephalus, defined as disproportionate increase in cerebrospinal fluid (CSF) within the cranium. It occurs in 3-4 per 1000 births and can be congenital or acquired. There are two main types - communicating and non-communicating - depending on whether CSF circulation or absorption is impaired. Clinical manifestations vary by age but include head enlargement, irritability, vomiting, and neurological deficits. Diagnosis involves measuring head growth curves and imaging tests like CT and MRI to identify ventricle size and site of obstruction.