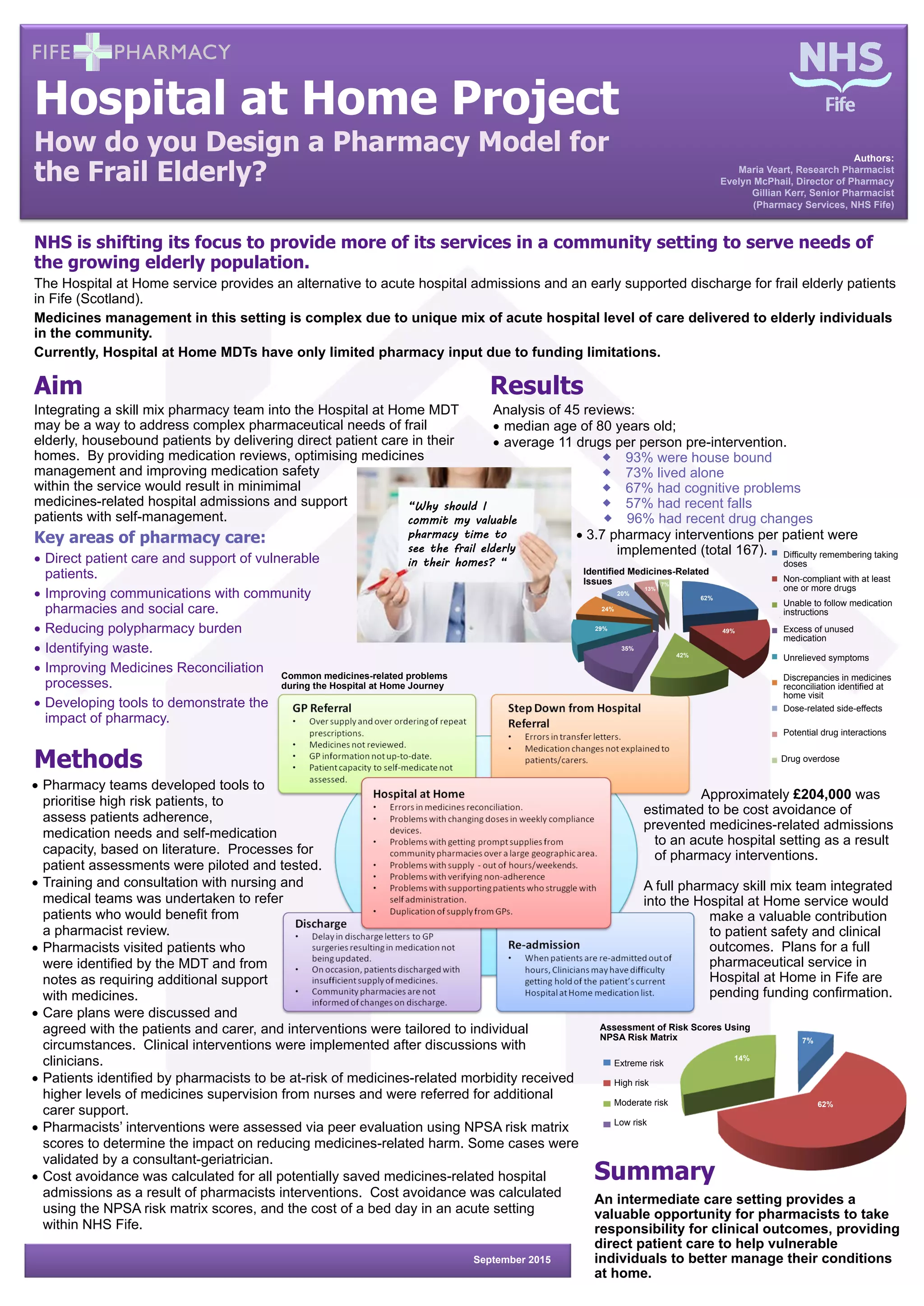
This document describes a study evaluating the impact of integrating pharmacists into a Hospital at Home service in Fife, Scotland. Pharmacists conducted medication reviews for 45 frail elderly patients in their homes, identifying 167 interventions. Common issues identified included difficulty remembering doses and non-compliance. The pharmacist interventions were estimated to avoid approximately £204,000 in costs from prevented medicines-related hospital admissions. Integrating pharmacists fully into the Hospital at Home service could improve patient safety and clinical outcomes for vulnerable elderly patients receiving acute care at home.