Recommended

Recommended
More Related Content
What's hot
What's hot (19)
Similar to HIV Salvage Therapy (Holden Young - Roseman University of Health Sciences)
Similar to HIV Salvage Therapy (Holden Young - Roseman University of Health Sciences) (20)
More from HoldenYoung3
More from HoldenYoung3 (17)
Recently uploaded
Recently uploaded (20)
HIV Salvage Therapy (Holden Young - Roseman University of Health Sciences)
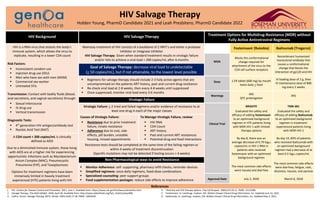
- 1. HIV Salvage Therapy Holden Young, PharmD Candidate 2021 and Leah Presbitero, PharmD Candidate 2022 HIV Background HIV Salvage Therapy Treatment Options for Multidrug-Resistance (MDR) without Fully Active Antiretroviral Regimens HIV is a RNA virus that attacks the body’s immune system, which allows the virus to replicate, resulting in a lower CD4 count Risk Factors: Inconsistent condom use Injection drug use (IDU) Men who have sex with men (MSM) Commercial sex worker Untreated STIs Transmission: Contact with bodily fluids (blood, anal secretions, and vaginal secretions) through: Sexual intercourse IV drug use Vertical transmission Diagnostic Tests: 4th generation HIV antigen/antibody test Nucleic Acid Test (NAT) Mainstay treatment of HIV consists of a backbone of 2 NRTI’s and either a protease inhibitor or integrase inhibitor HIV Salvage Therapy: Given when standard treatment results in virologic failure and/or fails to achieve a viral load < 200 copies/mL after 6 months Fostemsavir (Rukobia) Ibalizumab (Trogarzo) MOA Blocks the conformational change required for attachment of the virus to the CD4 cell surface receptors Recombinant humanized monoclonal antibody that causes a conformational change that blocks the interaction of gp120 and HIV Goal of Salvage Therapy: decrease viral load to undetectable (< 50 copies/mL), but if not attainable, to the lowest level possible Regimens for salvage therapy should include 2-3 fully active agents that are uncompromised on the patients ART history, past and current drug resistance Re-check viral load at 2-8 weeks, then every 4-8 weeks until suppressed Once suppressed, monitor viral load every 3-6 months Dose 1 ER tablet (600 mg) by mouth twice daily + food IV loading dose of 2 g, then IV maintenance dose of 800 mg every 2 weeks Warnings IRIS QTC prolongation IRIS Virologic Failure Virologic Failure: > 2 tried and failed regimens and/or evidence of resistance to at least one drug in each of the major classes Clinical Trial BRIGHTE Evaluated the safety and efficacy of adding fostemsavir to an optimized background regimen in HTE patients living with MDR HIV-1 with limited therapy options By day 8, there was an average decrease of 0.79 log10 copies/mL in HIV-1 RNA in patients who received fostemsavir with an optimized background regimen The most common side effects were nausea and diarrhea TMB-301 Evaluated the safety and efficacy of adding ibalizumab to an optimized background regimen in treatment- experienced patients living with MDR HIV-1 By day 14, 83% of patients who received ibalizumab with an optimized background regimen had a decrease of at least 0.5 log10 copies/mL The most common side effects were diarrhea, fatigue, rash, dizziness, nausea, and pyrexia Causes of Virologic Failure: Resistance due to prior treatment failure, innate resistance Adherence due to cost, side effects, pill burden, unstable housing, missed appointments To Manage Virologic Failure, review: HIV RNA CD4 Count ART history Past and current ART resistances Potential drug and food interactions A CD4 count < 200 copies/mL is clinically defined as AIDS Due to a diminished immune system, those living with AIDS are at a higher risk for experiencing opportunistic infections such as Mycobacterium Avium Complex (MAC), Pneumocystis Pneumonia (PJP), and Toxoplasmosis Options for treatment regimens have been immensely limited in heavily treatment experienced (HTE) patients living with HIV Resistance tests should be completed at the same time of the failing regimen or within 4 weeks of treatment discontinuation (Specific mutations may not be detected if testing occurs > 4 weeks) Non-Pharmacological ways to avoid Resistance Monitor Adherence: self- supporting, pharmacy refill checks, reminder devices Simplified regimens: once-daily regimens, fixed-dose combinations Specialized counseling: peer support groups Food supplementation packages: reduce side effects to improve adherence Approval Date July 2, 2020 March 6, 2018 References 1. HIV. Centers for Disease Control and Prevention. 2021, June 1. Available from: https://www.cdc.gov/hiv/basics/whatishiv.html 2. Salvage Therapy. The AIDS InfoNet. 2018, April 30. Available from: http://www.aidsinfonet.org/fact_sheets/view/408. 3. Collins, Simon. Salvage Therapy. BETA. Winter 2003;15(4):17-28. PMID: 12691034 4. Third line anti-HIV therapy options. Proj Inf Perspect. 2004;(37):19-21. PMID: 15119286 5. Fostemsavir. In: LexiDrugs. Hudson, OH: Wolters Kluwer Clinical Drug Information, Inc. Updated June 13, 2021. 6. Ibalizumab. In: LexiDrugs. Hudson, OH: Wolters Kluwer Clinical Drug Information, Inc. Updated May 3, 2021.