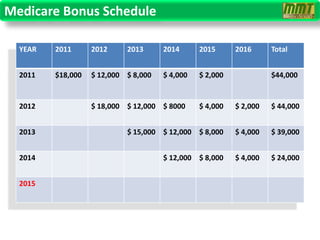
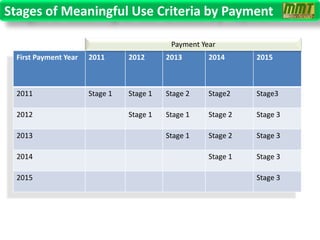
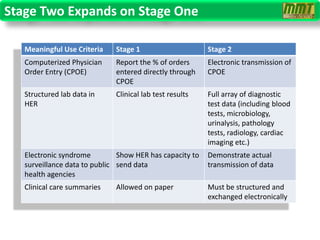
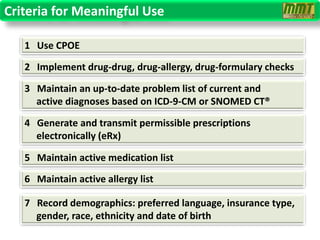
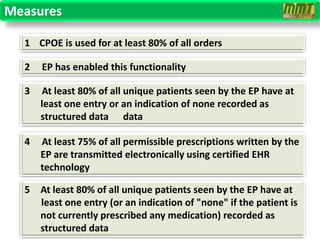
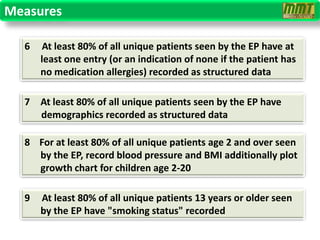
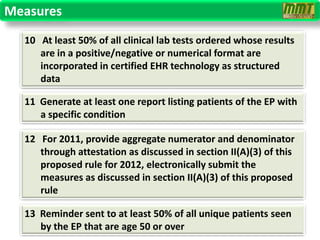
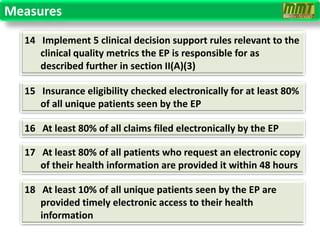
The document discusses the HITECH Act and the criteria for meaningful use of electronic health records (EHRs) in order to qualify for Medicare and Medicaid reimbursement bonuses starting in 2011. It outlines three stages of meaningful use criteria that providers must meet over multiple years to receive incentive payments. Stage one focuses on basic EHR usage and data capture, while stages two and three emphasize more advanced usage like clinical decision support and electronic data sharing. The criteria become more stringent over time to encourage higher levels of EHR utilization.