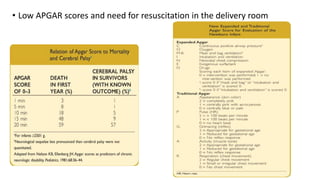
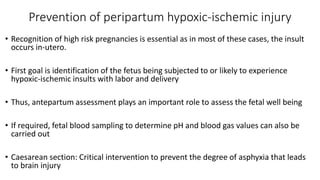
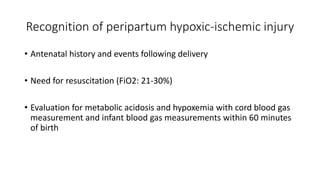
This document provides information on hypoxic ischemic encephalopathy (HIE) including its diagnosis, history, neurological examination, grading systems, laboratory and neuroimaging evaluation, and management. Key points include: HIE is diagnosed based on history, examination, and investigations showing metabolic derangements; risk factors include impairments of maternal/placental oxygenation or blood flow; neurological examination over the first week provides prognostic information; grading systems exist to determine severity; EEG and MRI can help determine injury site and prognosis; and management focuses on prevention, stabilization, and potential neuroprotective therapies.








![NEUROPROTECTIVE AGENTS
1) Anticonvulsant drugs such as phenobarbitone, topiramate have
neuroprotective action along with anticonvulsant action
[Silverstein FS, Barks JD. Combining hypothermia with other therapies for neonatal neuroprotection. In: Edwards AD, Azzopardi DV,
Gunn AJ, eds. Neonatal Neural Rescue: A Clinical Guide. New York: Cambridge University Press; 2013:208-218]
2) Xenon:
- Potent anesthetic, crosses BBB, leads to rapid induction of anesthesia
- Neuroprotective effects in combination with TH
- Studies show administration of Xenon unlikely to enhance neuroprotective effect
of cooling after birth asphyxia
[Hobbs C, Thoresen M, Tucker A, et al. Xenon and hypothermia combine additively, offering long-term functional and histopathologic
neuroprotection after neonatal hypoxia/ischemia. Stroke. 2008;39:1307-1313
Azzopardi D, Robertson NJ, Bainbridge A, et al. Moderate hypothermia within 6 h of birth plus inhaled xenon versus moderate
hypothermia alone after birth asphyxia (TOBY-Xe): a proof-of-concept, open-label, randomised controlled trial. Lancet Neurol.
2016;15:145-153]](https://image.slidesharecdn.com/hie-221122135638-a1082026/85/HIE-pptx-69-320.jpg)
![3) Antioxidants:
- Protect against oxidative stress which causes neonatal hypoxic-ischemic
injury
• N-Acetylcysteine:
- Crosses BBB, beneficial effect in combination with TH
[Jatana M, Singh I, Singh AK, et al. Combination of systemic hypothermia and N-acetylcysteine attenuates hypoxic–ischemic brain injury
in neonatal rats. Pediatr Res. 2006;59:684-689]
• Allopurinol:
- Xanthine oxidase inhibitor, free radical scavenger, has neuroprotective
properties
- Beneficial effect on free radical formation, cerebral hemodynamics and
electrical brain activity
[van Bel F, Shadid M, Moison RMW, et al. Effect of allopurinol on postasphyxial free radical formation, cerebral hemodynamics,
and electrical brain activity. Pediatrics. 1998;101:184-193
Chaudhari T, McGuire W. Allopurinol for preventing mortality and morbidity in newborn infants with suspected hypoxic-
ischaemic encephalopathy. Cochrane Database Syst Rev. 2008;(2):CD006817]](https://image.slidesharecdn.com/hie-221122135638-a1082026/85/HIE-pptx-70-320.jpg)
![4) Melatonin:
- Endogenous indolamine promising effect in treatment of HIE
- Antioxidant, anti-inflammatory, anti-apoptotic properties
- Freely crosses BBB
- In combination with TH: decreases oxidative stress, improved survival
with favorable neurodevelopmental outcome
- Optimal dose, route, duration of administration: under study
[Alonso-Alconada D, Alvarez A, Arteaga O, et al. Neuroprotective effect of melatonin: a novel therapy against perinatal
hypoxiaischemia. Int J Mol Sci. 2013;14:9379-9395
Robertson NJ, Faulkner S, Fleiss B, et al. Melatonin augments hypothermic neuroprotection in a perinatal asphyxia model.
Brain. 2013;136:90-105]](https://image.slidesharecdn.com/hie-221122135638-a1082026/85/HIE-pptx-71-320.jpg)
![5) Erythropoietin:
- Neuroprotective action in terms, preterms
- Glycoprotein, involved in adaptive response to perinatal hypoxia-ischemia
- Principal sequence:
Hypoxia induces hypoxia-inducible factor increased expression of EPO and its
receptors in neurons, astrocytes, oligodendroglia, microglia, endothelial cells
- Principal neuroprotective mechanisms:
Anti-excitotoxic, anti-oxidant, anti-inflammatory , anti-apoptotic
- Decreases risk of brain injury after HI
- Synergistic neuroprotective effect with TH
- Prolonged EPO therapy: maybe effective in reparative and restorative mechanisms
- Promotes neurogenesis, oligodendroglial development, angiogenesis
[Xiong T, Qu Y, Mu D, et al. Erythropoietin for neonatal brain injury: opportunity and challenge. Int J Dev Neurosci. 2011;29:583-591
Zhu C, Kang W, Xu F, et al. Erythropoietin improved neurologic outcomes in newborns with hypoxic–ischemic encephalopathy. Pediatrics.
2009;124:e218-e226]](https://image.slidesharecdn.com/hie-221122135638-a1082026/85/HIE-pptx-72-320.jpg)
![6) Magnesium sulphate:
- Tocolytic for preterm labor, treatment for pre eclampsia
- Has shown neuroprotective effect in some studies
- But no reliable data to suggest antenatal MgSO4 prevents preterm brain
injury
[Galinsky R, Bennet L, Groenendaal F, et al. Magnesium is not consistently neuroprotective for perinatal hypoxia-ischemia in
term-equivalent models in preclinical studies: a systematic review. Dev Neurosci. 2014;36:73-82.
Tagin M, Shah PS, Lee KS. Magnesium for newborns with hypoxic–ischemic encephalopathy: a systematic review and meta-
analysis. J Perinatol. 2013;33:663-669]
7) Calcium channel blockers:
- Increased Ca influx Increase cytosolic Ca Neuronal death
- Thus, CCB may be beneficial in preventing this cascade, but not yet proved
[Levene MI, Gibson NA, Fenton AC, et al. The use of a calciumchannel blocker, nicardipine, for severely asphyxiated newborn
infants. Dev Med Child Neurol. 1990;32:567-574]](https://image.slidesharecdn.com/hie-221122135638-a1082026/85/HIE-pptx-73-320.jpg)
![8) Stem cell therapy:
- Role in neuroprotection, neurorestoration
- Human cord blood, multipotent stem cells, progenitor cells, neural stem
cells can be used
- Anti-apoptotic, anti-inflammatory effects
- Autologous, volume and RBC-reduced human cord blood has been used:
safe and feasible
[Liao Y, Cotten M, Tan S, et al. Rescuing the neonatal brain from hypoxic injury with autologous cord blood. Bone Marrow Transplant.
2013;48:890-900
Cotten CM, Murtha AP, Goldberg RN, et al. Feasibility of autologous cord blood cells for infants with hypoxic–ischemic encephalopathy.
J Pediatr. 2014;164:973-979.e971]
9) Others:
- Caspase inhibitors - Cannabinoids
- IGF-1 - Osteopontin](https://image.slidesharecdn.com/hie-221122135638-a1082026/85/HIE-pptx-74-320.jpg)