This document provides an overview of hematology, including:
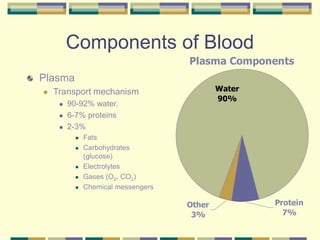
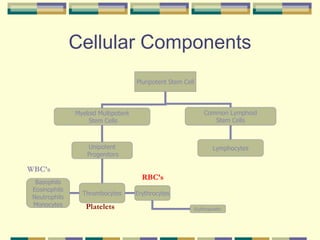
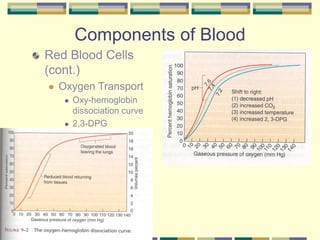
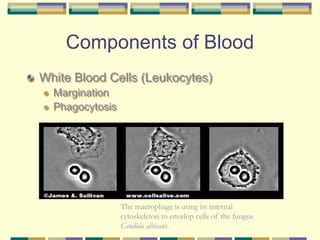
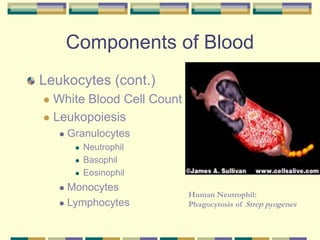
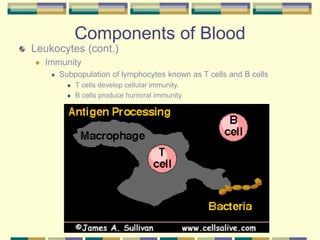
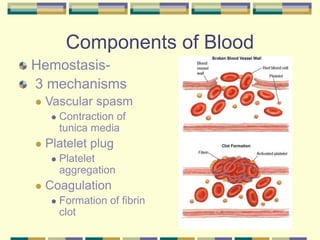
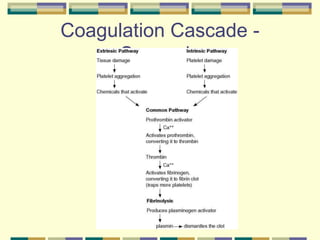
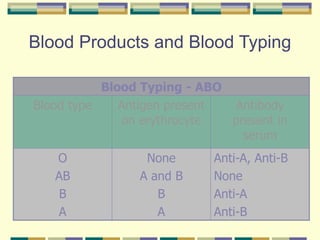
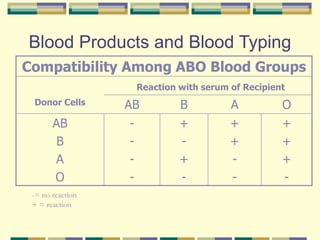
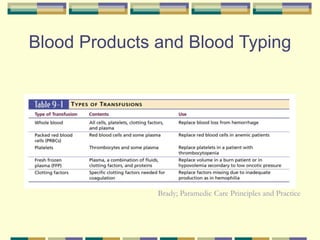
1) The components of blood such as red blood cells, white blood cells, platelets, and plasma. It describes blood typing and the coagulation cascade.
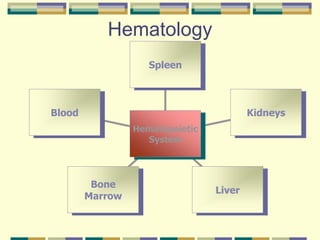
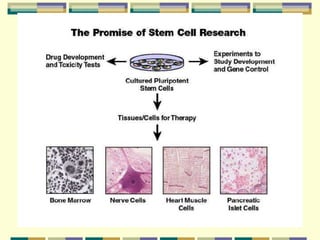
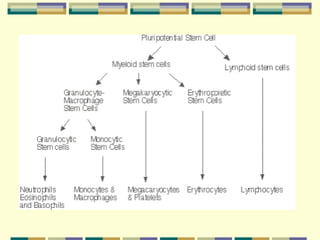
2) Hematopoiesis, the process of blood cell production, and the roles of stem cells, growth factors, and the bone marrow microenvironment.
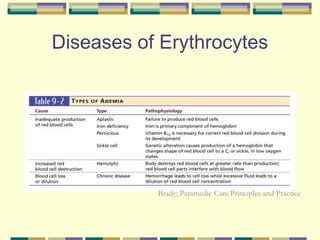
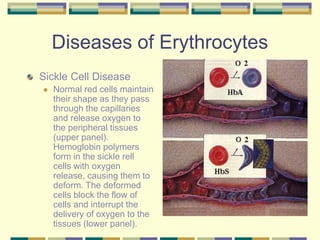
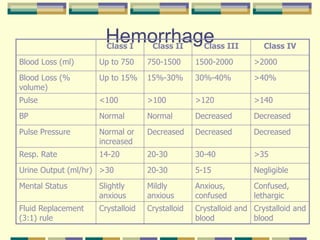
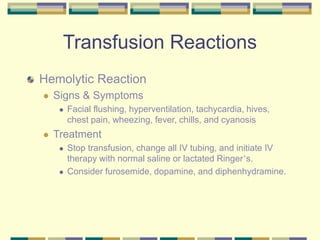
3) Common hematological diseases like anemias, sickle cell disease, polycythemia, leukemias, and clotting disorders. It discusses associated signs/symptoms and general management approaches.








































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


















