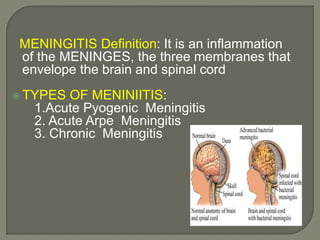
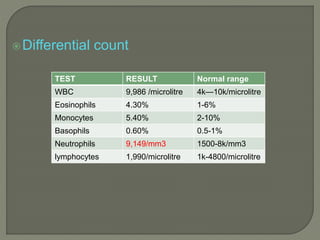
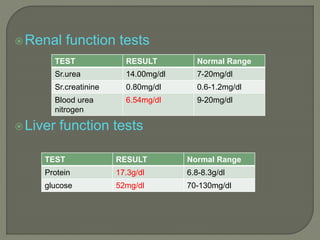
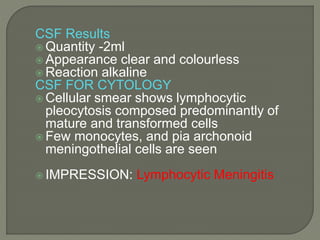
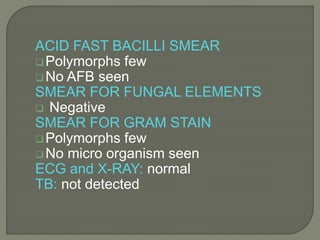
Meningitis is an inflammation of the meninges, the membranes surrounding the brain and spinal cord. There are different types including acute pyogenic and acute arpe meningitis. Symptoms include severe headache, neck stiffness, fever, vomiting, sensitivity to light and sound. Diagnosis involves lumbar puncture to examine cerebrospinal fluid for increased white blood cells, protein levels and decreased glucose. The patient presented with headache and fever and was diagnosed with acute meningitis based on clinical findings and CSF analysis showing lymphocytic pleocytosis. Treatment involved antibiotics, antivirals, analgesics and other supportive medications.

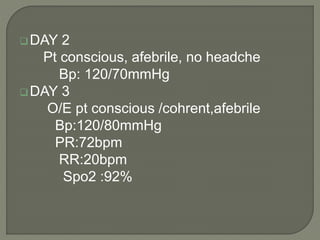
![1. CSF-Lumbar puncture L3-L4 and L4-L5 –
cloudy appearance/purulent
2. Increase in Neutrophils[90,000/mm3]
3.Increase in Protein level[>100 or500]
4.Decrease Glucose levels [<50%]
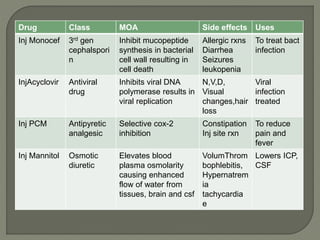
Ranges in meningitis:
Lymphocyte Protein Glucose
Bacteria 50-2000 1-3 <50%
TB 100-600 1-6 <50%
Viral 5-500 0.5-1 Normal
Fungal 50-1000 1-3 <50%](https://image.slidesharecdn.com/hema1-200716125746/85/Hema-1-7-320.jpg)
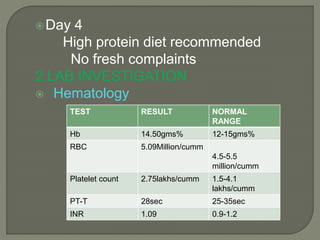
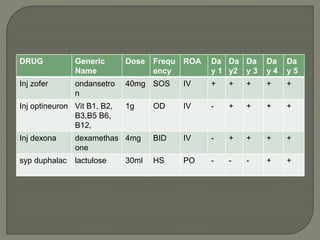
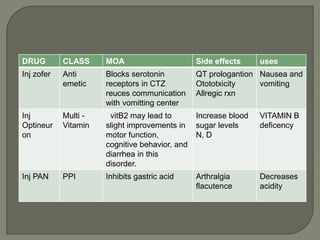
![Drug class MOA Side effects Uses
Inj Dexona corticosteroid unclear HTN,
Dyspepsia
Cataract(10%
)
Regulate
inflammation
response and
cover CSF
pressure
Syp Duphalac Laxative Increase in
stool water
and soft stool
[bcoz
constipation
may lead to
fever]
Bleaching
Excessive
bowel activity
Treat
constipation](https://image.slidesharecdn.com/hema1-200716125746/85/Hema-1-21-320.jpg)