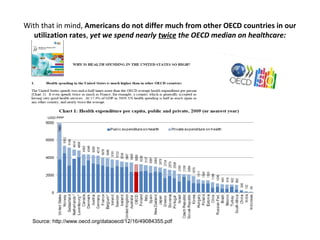
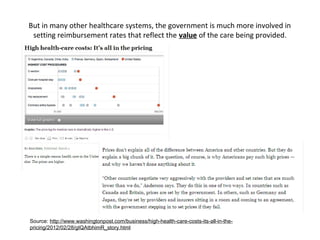
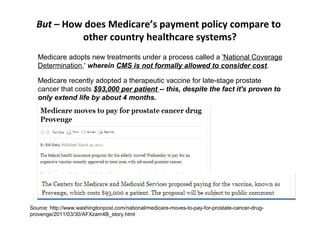
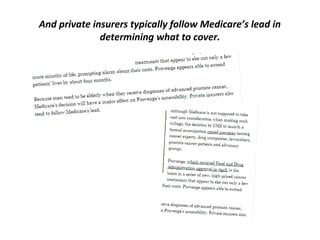
The document critiques the inefficiency of the American healthcare system, highlighting the significant cost disparity compared to other OECD countries without corresponding improvements in health outcomes. It advocates for reforms including high-deductible consumer-driven health plans, greater price transparency, and the integration of comparative-effectiveness research into Medicare payment policies to promote value and control spending. Ultimately, the document suggests that targeted policy changes could align healthcare spending with quality care and improve the system's sustainability.