Downloaded 10 times
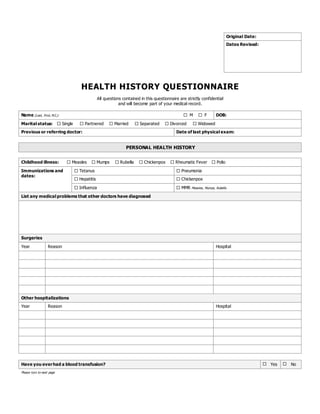
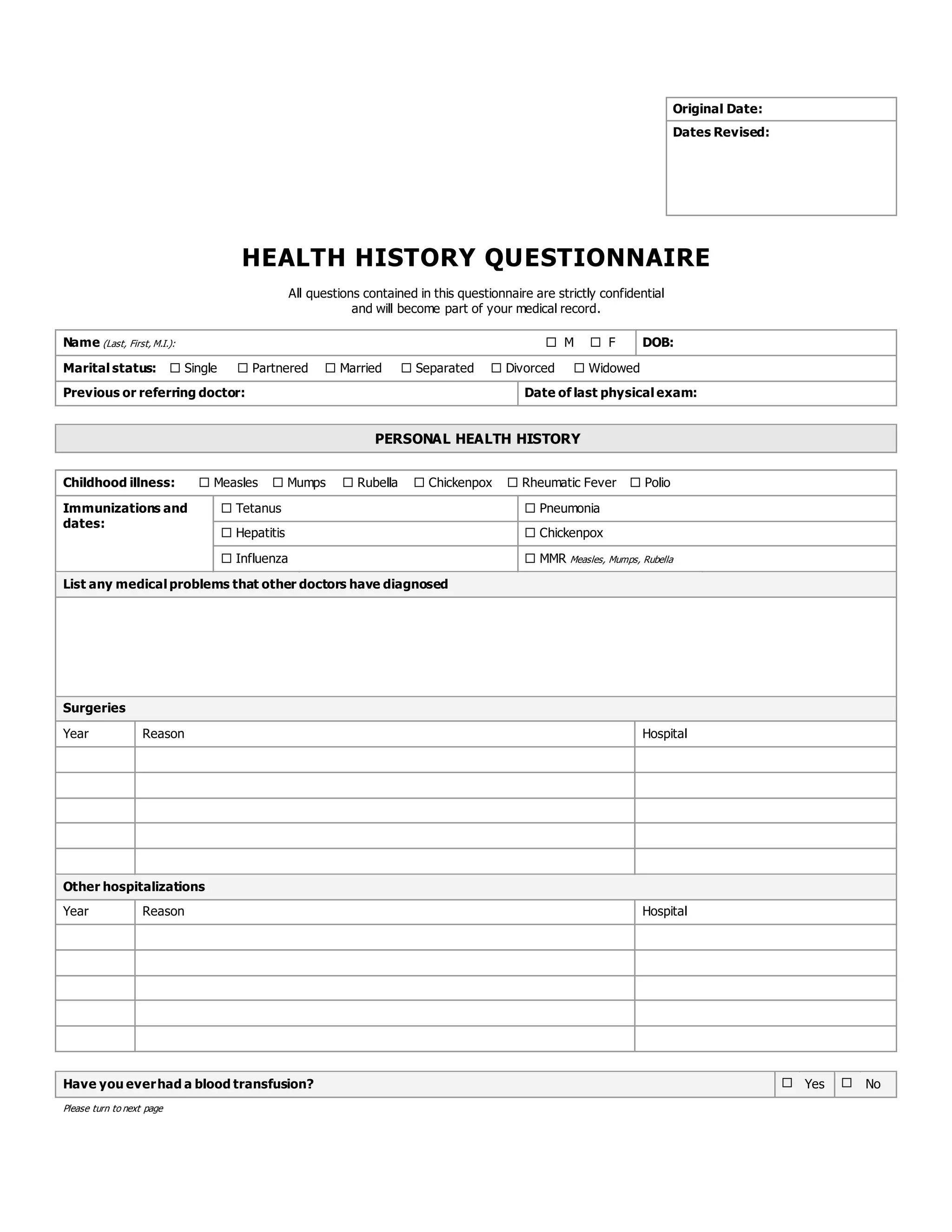
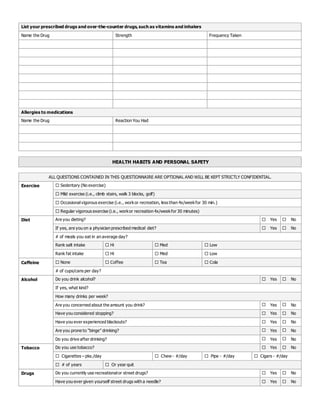



This document contains a health history questionnaire that collects personal and family medical history information. It asks about childhood illnesses, surgeries, medications, allergies, health habits like exercise, diet, alcohol and tobacco use, as well as mental health, women's health, and men's health questions. The questionnaire is confidential and will become part of the patient's medical record.























































































