H2 s injuries you are not listening
•
0 likes•436 views

H2S injuries in the workplace you are not listening to the safety rules

Recommended
More Related Content
What's hot
What's hot (20)
Similar to H2 s injuries you are not listening
Similar to H2 s injuries you are not listening (20)
More from Terry Penney
More from Terry Penney (20)
Recently uploaded
Recently uploaded (20)
H2 s injuries you are not listening
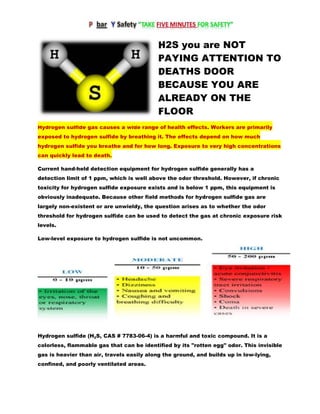
- 1. H2S you are NOT PAYING ATTENTION TO DEATHS DOOR BECAUSE YOU ARE ALREADY ON THE FLOOR Hydrogen sulfide gas causes a wide range of health effects. Workers are primarily exposed to hydrogen sulfide by breathing it. The effects depend on how much hydrogen sulfide you breathe and for how long. Exposure to very high concentrations can quickly lead to death. Current hand-held detection equipment for hydrogen sulfide generally has a detection limit of 1 ppm, which is well above the odor threshold. However, if chronic toxicity for hydrogen sulfide exposure exists and is below 1 ppm, this equipment is obviously inadequate. Because other field methods for hydrogen sulfide gas are largely non-existent or are unwieldy, the question arises as to whether the odor threshold for hydrogen sulfide can be used to detect the gas at chronic exposure risk levels. Low-level exposure to hydrogen sulfide is not uncommon. Hydrogen sulfide (H2S, CAS # 7783-06-4) is a harmful and toxic compound. It is a colorless, flammable gas that can be identified by its "rotten egg" odor. This invisible gas is heavier than air, travels easily along the ground, and builds up in low-lying, confined, and poorly ventilated areas.
- 2. Naturally occurring sources include decaying plants, animals, and sewage, usually at low oxygen conditions. It occurs in mines, springs, sewers, swamps, volcanoes, and fossil fuels. Industrial sources include petroleum and natural gas extraction, petroleum refining, paper manufacturing, leather tanning, chemical manufacturing, and waste disposal. Hydrogen sulfide has a low odor threshold, and its smell may be detected below 1 ppm. The minimal perceptible odor is reported as 0.13 ppm. The rotten egg odor is recognizable up to 30 ppm. It has a sweet odor at 30 ppm to 100 ppm. At concentrations above 100 ppm, detection ability is affected by rapid temporary paralysis of the olfactory nerves, resulting in loss of the sense of smell. H2S is a chemical asphyxiant and mitochondrial poison. Its behavior through inhalation exposure is similar to cyanide and carbon monoxide, which prevent the use of oxygen.
- 3. OH&S established an eight-hour permissible exposure limit-time weighted average (PEL-TWA) of 10 ppm and a 15-minute short-term exposure limit (PEL-STEL) of 15 ppm for exposed workers. NIOSH established a limit of 300 ppm as the immediately dangerous to life and health concentration. What about longer term health effects? Some people who breathed in levels of hydrogen sulfide high enough to become unconscious continue to have headaches and poor attention span, memory, and motor function after waking up. Problems with the cardiovascular system have also been reported at exposures above permissible exposure limits. People who have asthma may be more sensitive to hydrogen sulfide exposure. That is, they may have difficulty breathing at levels lower than people without asthma. The explosive range of hydrogen sulfide in air is 4.5 to 45.5 percent. This range is much higher than the PEL. Safety Hazards Hydrogen sulfide is a highly flammable, explosive gas, and can cause possible life-threatening situations if not properly handled. In addition, hydrogen sulfide gas burns and produces other toxic vapors and gases, such as sulfur dioxide. In addition to exposure to hydrogen sulfide in the air, exposure to liquid hydrogen sulfide can cause "blue skin" or frostbite. If clothing becomes wet, avoid ignition sources, remove the clothing and isolate it in a safe area to allow it to evaporate. The effect called knockdown (rapid unconsciousness) often results in falls that can seriously injure the worker.
- 4. FIRST AID TREATMENT IF IMMEDIATE HELP IS AVAILABLE Initial treatment of hydrogen sulfide exposure requires immediate removal of the victim from the contaminated area into a ventilated/fresh-air environment. Prehospital care providers should take hazardous materials precautions with respirator devices (self-contained breathing apparatus [SCBA]) to avoid serious exposure. Protected rescue personnel can measure the environmental concentration of hydrogen sulfide, providing an initial clue to the diagnosis. In severe cases, intubation may be necessary for ventilatory support and airway protection. Establish intravenous (IV) access or initiate other initial supportive care as necessary. Search the patient's pockets for discolored copper coins, which can be an early diagnostic clue. In the emergency department, high-flow (100%) oxygen is the mainstay of therapy for hydrogen sulfide poisoning. Supportive therapy includes aggressive ventilation and possible use of positive pressure ventilation for the patients with evidence of acute lung injury. IV fluids and vasopressors should be administered to hypotensive patients. Correction of acidosis based on arterial blood gas and serum lactate values is indicated. Based on the similarities in cyanide and hydrogen sulfide toxicity, induced methemoglobinemia may be used in hydrogen sulfide toxicity. Methemoglobin acts as a scavenger, and it has a stronger affinity to hydrogen sulfide than to cytochrome oxidase. Administer 10 mL of 3% sodium nitrite IV over 2-4 minutes (adult dose). Obtain a methemoglobin level 30 minutes after administration of antidote. Patients who have suffered significant exposure (ie, anything other than chronic low- level exposure with mucous membrane irritation) should be admitted to the intensive care unit. Patients who are unresponsive to intravenous nitrites or who have persistent or delayed neurologic sequelae should be considered for hyperbaric oxygen therapy (HBO). Anecdotal reports indicate a salutary effect.