Downloaded 45 times











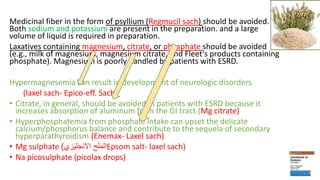























![• Conclusions: Use of PPIs in patients dialyzed using a dialysate [Mg] of 0.75-
1.0 mEq/l is associated with hypomagnesemia. We suggest monitoring
plasma [Mg] in patients taking PPIs, with discontinuation of the medication
if possible and/or adjustment of dialysate [Mg] to normalize plasma [Mg].](https://image.slidesharecdn.com/gitinhd-161223220001/85/GIT-in-Hemodialysis-36-320.jpg)













1. Gastrointestinal symptoms are common among hemodialysis patients and include nausea, vomiting, abdominal pain, dyspepsia, constipation, and diarrhea. The causes are often multifactorial related to uremia, dialysis treatment, and medications. 2. Abdominal pain in dialysis patients can be caused by various gastrointestinal or non-gastrointestinal issues. Common gastrointestinal causes include diseases of the upper gastrointestinal tract, lower gastrointestinal tract, hepatobiliary system, and pancreas. Non-gastrointestinal causes include metabolic, hematologic, cardiovascular/pulmonary, endocrine, neurological, and toxic disorders. 3. Dialysis patients may be at increased risk for gastrointestinal



































































































