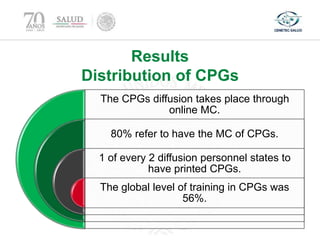
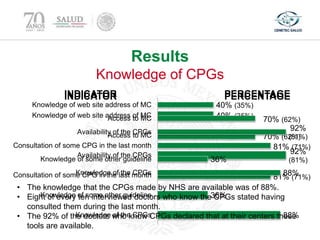
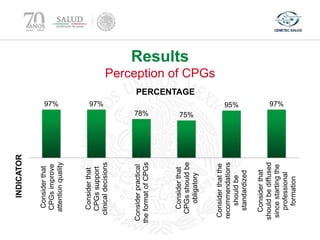
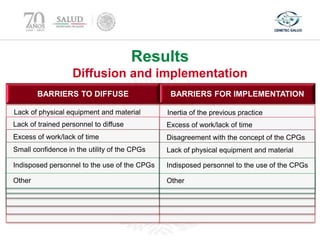
This document evaluates the success of clinical practice guideline (CPG) diffusion and implementation in Mexico's National Health System. A survey of 480 randomly sampled primary and secondary health centers found that 80% reported access to CPGs online, but only half had printed copies. Overall CPG training was 56%. While knowledge and perception of CPGs was generally positive, barriers to effective implementation included lack of resources, training, and time. The study concludes that CPG distribution is good but implementation varies and requires further work.