Download to read offline








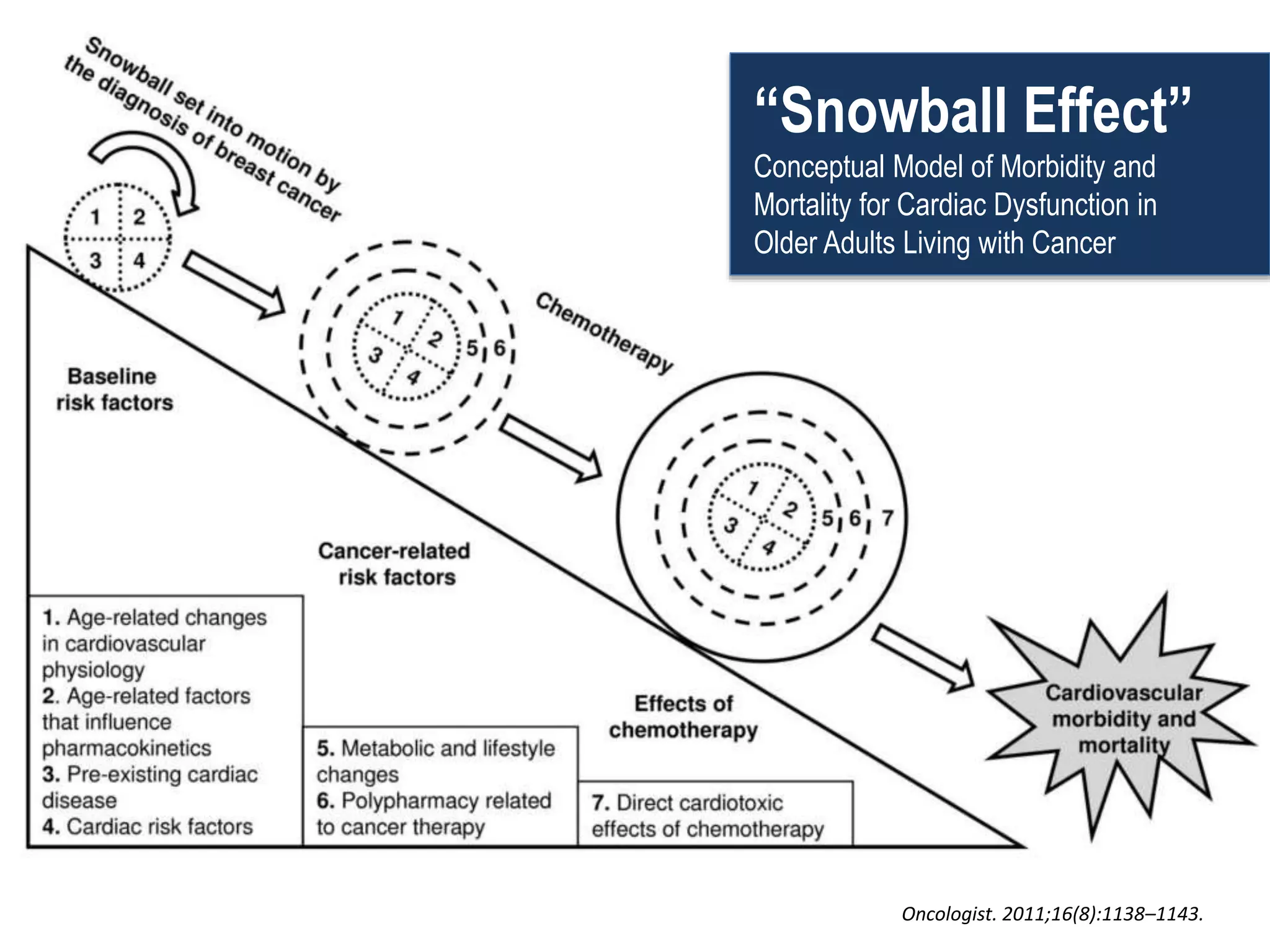
















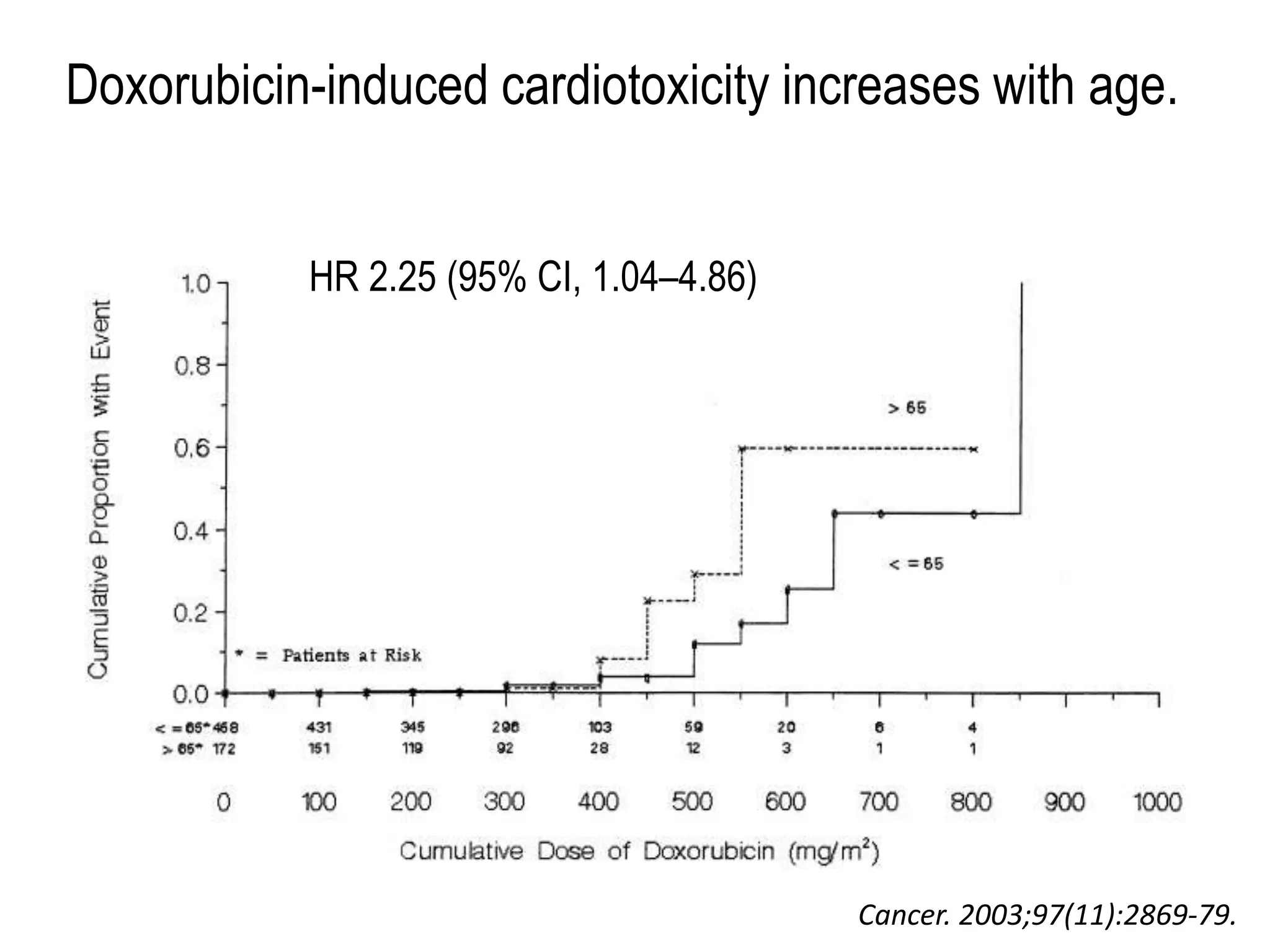
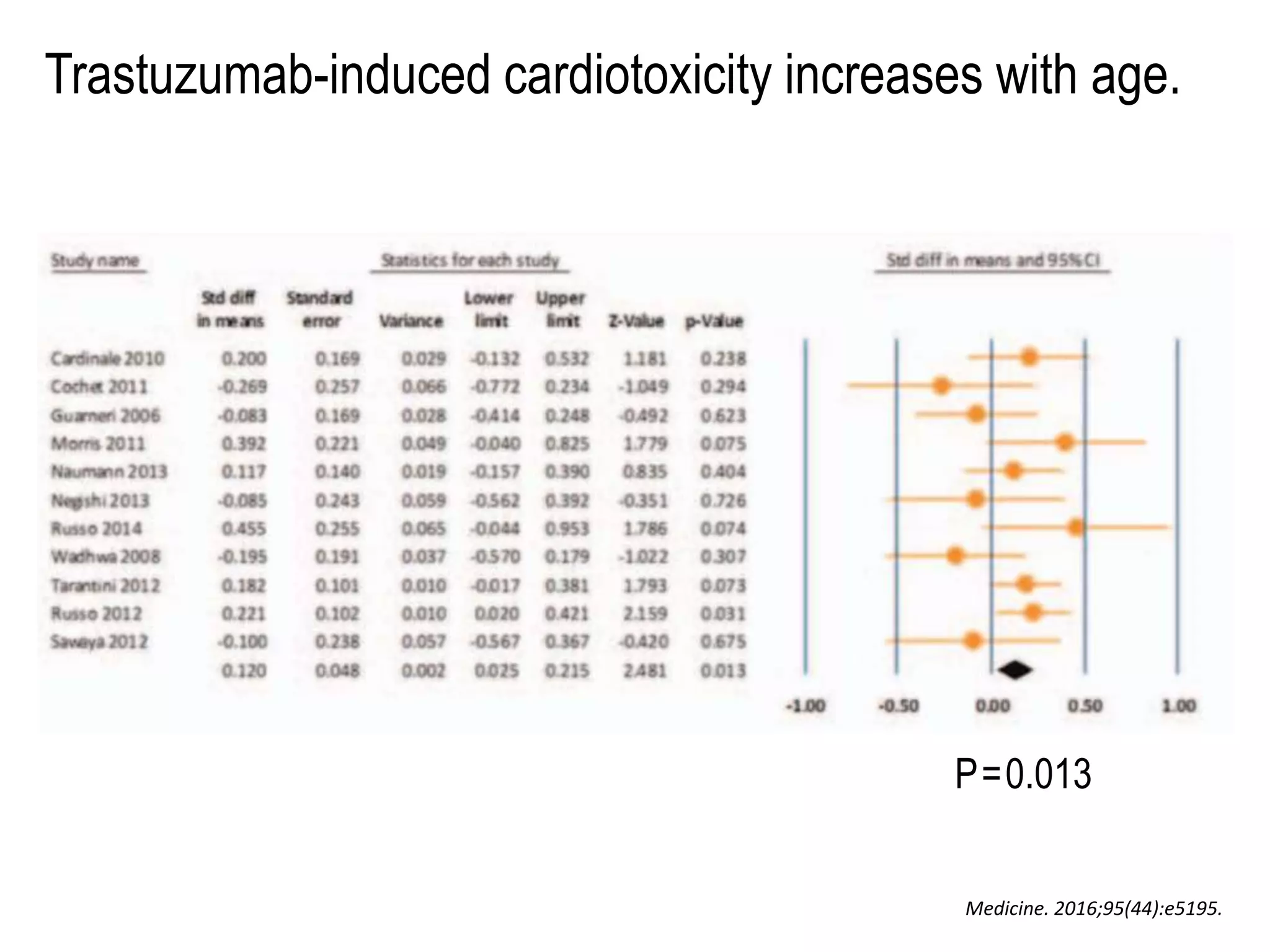
























This document discusses special considerations for cardiac dysfunction in older adults living with cancer. It begins with objectives to apply a framework for multimorbidity and review cardiovascular physiology of aging and considerations in cardio-oncology for older adults. It then discusses how chronic diseases increase with age, including cancer and heart disease. Older adults are underrepresented in oncology trials despite having high rates of cancer. A comprehensive geriatric assessment is recommended to identify vulnerabilities beyond standard oncology assessments. Certain chemotherapy agents have increased cardiotoxicity risks in older patients. A multimorbidity framework is presented to guide management of multiple chronic conditions. Strategies are discussed to minimize cardiac complications in older cancer patients, including risk stratification, cardioprotective therapies






























![OPEC [639] Managing Cancer Palliative Care of the Elderly Patient.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/opec639managingcancerpalliativecareoftheelderlypatient-251223183603-5922eac9-thumbnail.jpg?width=640&height=640&fit=bounds)



































