Downloaded 46 times










![“In ONCOLOGY, personalized treatment often begins with
the tumour, its pathology, genetics and staging, which are
incorporated in algorithms that yield treatment
recommendations; the next step will then be to assess
whether the patient is suitable for the treatment.
A GERIATRIC approach to personalized treatment often
starts at the other end, with an emphasis on the patient's
health status, individual goals of care and physical strengths
and limitations; subsequently, it is assessed whether the
treatment is suitable for the patient.”
J Geriatr Oncol. 2019. [Epub ahead of print]](https://image.slidesharecdn.com/nov12019-canadiangeriatriconcologyconference-191023170530/85/Geriatric-Oncology-49-320.jpg)



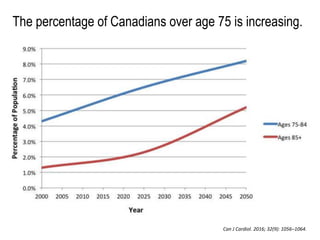
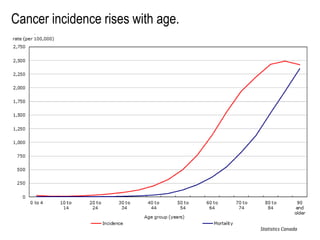
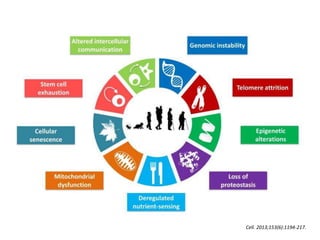
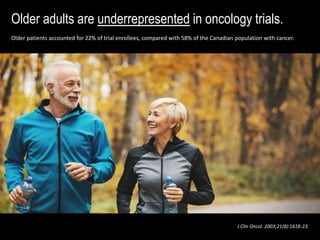
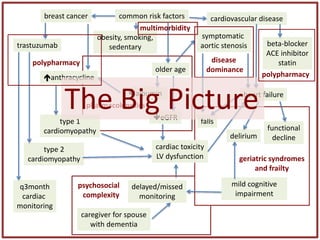
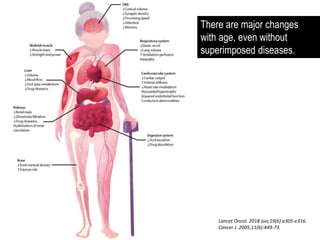
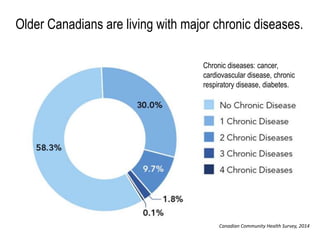
Dr. Camilla Wong's presentation at the annual geriatric oncology conference emphasizes the importance of geriatric assessments for older adults with cancer, outlining how aging and factors such as frailty and multimorbidity can significantly impact cancer management. The document highlights the underrepresentation of older patients in clinical trials and advocates for a more inclusive approach, enhancing the personalization of treatment plans by considering patients' health status and individual goals. Wong stresses the need for collaborative efforts in research and clinical practice to improve outcomes for older cancer patients.




































![OPEC [639] Managing Cancer Palliative Care of the Elderly Patient.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/opec639managingcancerpalliativecareoftheelderlypatient-251223183603-5922eac9-thumbnail.jpg?width=640&height=640&fit=bounds)