Download to read offline






![14
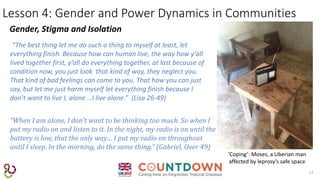
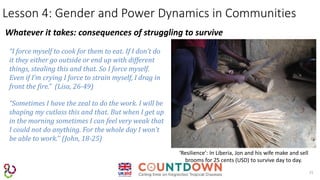
Lesson 4: Gender and Power Dynamics in Communities
Gender, Poverty and Abandonment
‘Abandonment’: In DRC, Neema
and her mother were abandoned
by their father and husband.
“When I was accused as witch craft- in 96, I received heavy beating,
excused me please….the switch that hit my nut seed [scrotum] it
caused me…I was out of my sex. In 2003, they took out the thing. I
just like that. So she too, she can’t be like that. So she went back to
her old husband.” (Gabriel, Over 49)
“You have no place to go. Then your family who will say come sit
down near me here. Now they say “go away from me”, then where
are you going to go?” (Emine, Over 49)](https://image.slidesharecdn.com/ileppresentationst-171026173329/85/Gender-and-Leprosy-Why-it-Matters-14-320.jpg)

![References
18
• Hogan, E. (2017) “An intersectional approach to the psycho-social burden of leprosy: A Liberian case study” Masters dissertation,
Liverpool School of Tropical Medicine. WHO. 2015. “What Do We Mean by ‘Sex’ and ‘Gender’?”
http://www.who.int/gender/whatisgender/en/ (May 4, 2015).
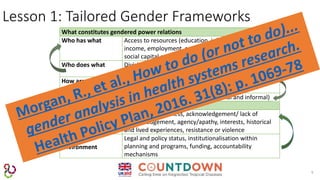
• Morgan, R., et al., How to do (or not to do)... gender analysis in health systems research. Health Policy Plan, 2016. 31(8): p. 1069-78
• Newman, Constance. 2014. “Time to Address Gender Discrimination and Inequality in the Health Workforce.” Human Resources for
Health 12(1): 25.
• Nowatzki, Nadine, and Karen R Grant. 2011. “Sex Is Not Enough: The Need for Gender-Based Analysis in Health Research.” Health
Care for Women International 32(4): 263–77.
• Ravindran, Sundari TK (2015). Health financing mechanisms in India and their implications for women’s access to health care
(presentation). In Health Systems Financing – What’s gender got to do with it?.
• Standing, Hilary. 1997. “Gender and Equity in Health Sector Reform Programmes: A Review.” Health Policy and Planning 12(1): 1–18.
• Simpon, J. (2009). Everyone Belongs: A Toolkit for Applying Intersectionality. [Intersectionality Wheel] Available at: http://www.criaw-
icref.ca/sites/criaw/files/Everyone_Belongs_e.pdf (Accessed 8 August 2017)
• WHO. 2015. “What Do We Mean by ‘Sex’ and ‘Gender’?” http://www.who.int/gender/whatisgender/en/ (May 4, 2015).](https://image.slidesharecdn.com/ileppresentationst-171026173329/85/Gender-and-Leprosy-Why-it-Matters-18-320.jpg)

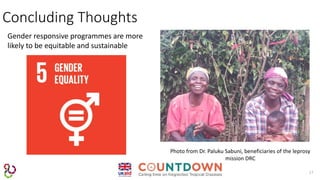
The document discusses the importance of understanding gender as a social construct that influences health systems, including access to care and health outcomes. It highlights lessons learned from gender mainstreaming in the context of leprosy, emphasizing the need for tailored gender frameworks, the impact of intersectionality, and the necessity of a critical gender lens in data collection. The authors argue that recognizing and addressing gender dynamics is vital for developing equitable and sustainable health policies.























































































