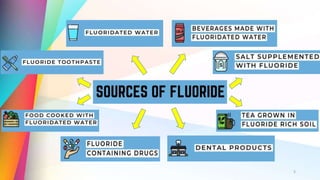
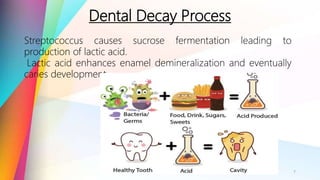
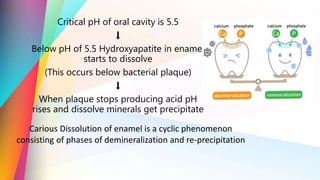
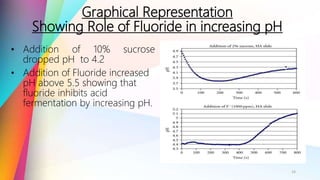
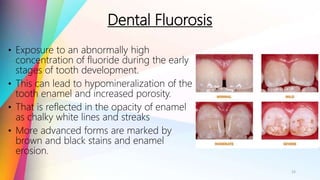
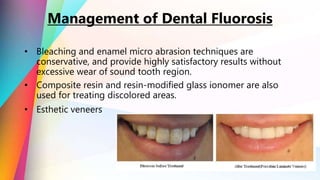
The document discusses the role of fluoride in dental biofilm and its importance in preventing dental decay through mechanisms like remineralization and inhibition of harmful bacteria. It highlights the mechanisms by which fluoride enhances enamel resistance and the consequences of excessive fluoride exposure, such as dental and skeletal fluorosis. The conclusion emphasizes the need for balanced fluoride intake to maximize its benefits while minimizing risks, supported by the Indian Dental Association.








































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)








