1. The debriefing checklist outlines steps for assessing a patient in labor and delivery, including taking a report, washing hands, introducing oneself, checking vitals, and performing a vaginal exam.
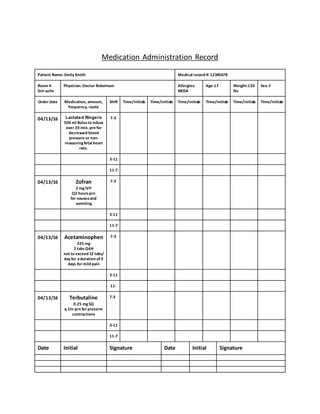
2. The nurse is to delegate tasks to an assistant nurse, such as obtaining supplies, starting an IV, drawing labs, and applying the fetal monitor.
3. Communication is important, with nurses verbalizing each task and reporting back findings to the patient and team.
4. A thorough patient assessment is conducted regarding contractions, fetal heart rate, medical and pregnancy history.