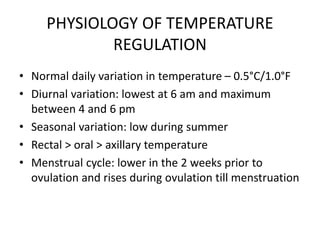
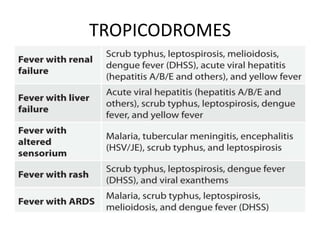
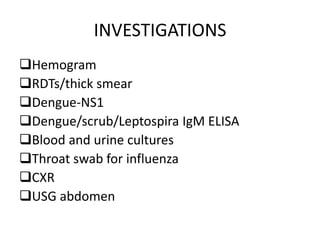
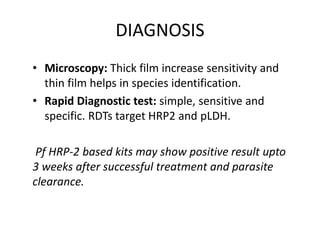
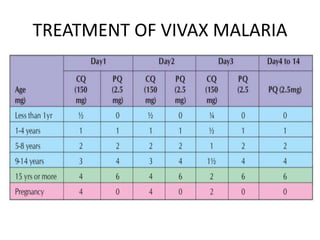
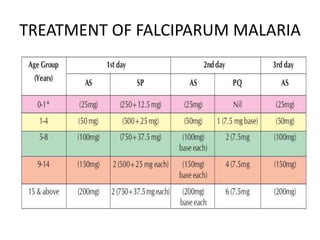
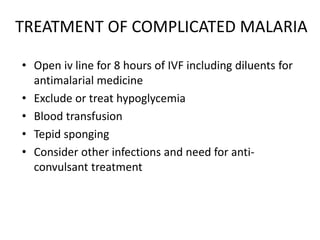
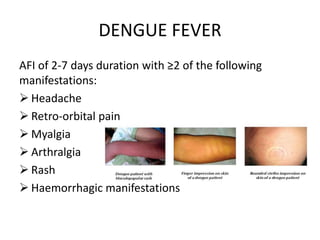
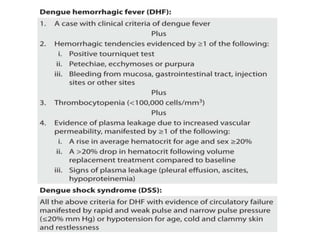
This document summarizes fever and febrile syndromes. It discusses the physiology of temperature regulation in the body and the pathogenesis of fever. It describes the different causes of fever including exogenous and endogenous pyrogens. It then discusses specific infectious causes of fever like malaria, enteric fever, dengue, leptospirosis, and scrub typhus. For each condition, it summarizes the causative organism, transmission, clinical features, diagnosis, and treatment. It also discusses complications, investigations, and management principles for febrile illnesses.
































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)











