Exercise and Chronic Kidney Disease Current Recommendations.pptx
1.
Exercise and ChronicKidney Disease
Current Recommendations
Michael Bruneau Jr. MS, ACSM EPC, NASM CPT
Springfield College, Springfield, MA
May 4th
, 2016
2.
Overview
• Staging ofCKD
• Prevalence of CKD
• Consequences of having CKD
• PA and mortality in CKD
• Exercise and CKD in predialysis patients
• Exercise and the progression of CKD
• Exercise and CVD in CKD
• Exercise and physical function in CKD
• Current recommendations
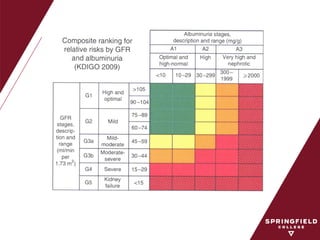
Staging of CKD
•Chronic kidney disease is defined as either
damage or a glomerular filtration rate < 60
mL/min/1.73m2
for 3 months
≧
• Kidney damage is defined as pathologic
abnormalities or markers of damage, including
abnormalities in blood or urine or imaging
studies
KDOQI Guidelines (2005)
5.
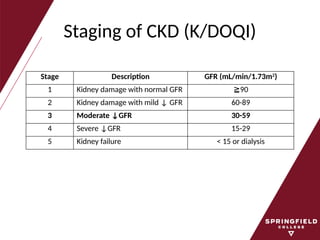
Staging of CKD(K/DOQI)
Stage Description GFR (mL/min/1.73m2
)
1 Kidney damage with normal GFR ≧90
2 Kidney damage with mild ↓ GFR 60-89
3 Moderate ↓GFR 30-59
4 Severe ↓GFR 15-29
5 Kidney failure < 15 or dialysis
7.
Treatments for ESRD
•Patient with ESRD have FOUR treatment
options:
– Hemodialysis (in center and home)
– Peritoneal dialysis (home)
– Kidney transplantation
– “Conservative management”
• No dialysis or transplant option often chosen by
frail elderly patients
Prevalence of CKD
•25 million people (~13.4%) in the United
States (US) have CKD
– Based upon estimates using albumin/creatinine
ratios (ACR), and GFR values
• Affects > 40% of people > 70 years of age
Levey et al. (2010)
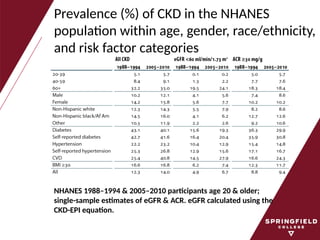
10.
Prevalence (%) ofCKD in the NHANES
population within age, gender, race/ethnicity,
and risk factor categories
NHANES 1988–1994 & 2005–2010 participants age 20 & older;
single-sample estimates of eGFR & ACR. eGFR calculated using the
CKD-EPI equation.
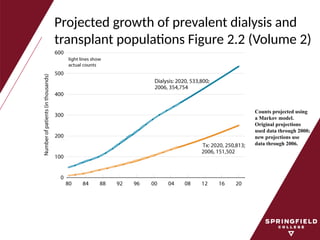
11.
Projected growth ofprevalent dialysis and
transplant populations Figure 2.2 (Volume 2)
Counts projected using
a Markov model.
Original projections
used data through 2000;
new projections use
data through 2006.
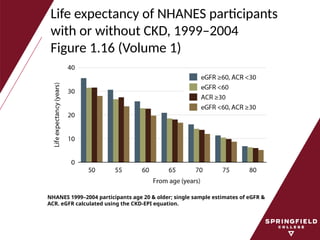
Life expectancy ofNHANES participants
with or without CKD, 1999–2004
Figure 1.16 (Volume 1)
NHANES 1999–2004 participants age 20 & older; single sample estimates of eGFR &
ACR. eGFR calculated using the CKD-EPI equation.
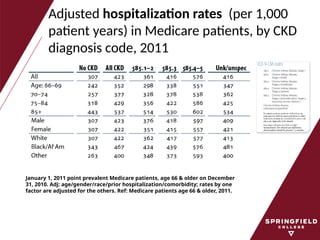
14.
Adjusted hospitalization rates(per 1,000
patient years) in Medicare patients, by CKD
diagnosis code, 2011
January 1, 2011 point prevalent Medicare patients, age 66 & older on December
31, 2010. Adj: age/gender/race/prior hospitalization/comorbidity; rates by one
factor are adjusted for the others. Ref: Medicare patients age 66 & older, 2011.
15.
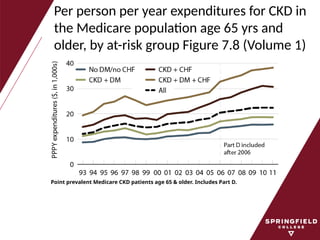
Per person peryear expenditures for CKD in
the Medicare population age 65 yrs and
older, by at-risk group Figure 7.8 (Volume 1)
Point prevalent Medicare CKD patients age 65 & older. Includes Part D.
16.
The Bottom Line
•CKD is a costly disease and its prevalence is
increasing
• CKD patients are at greater risk of dying
prematurely than progressing to ESRD
• Preliminary evidence has shown increased
fitness and physical activity levels may be
protective in CKD
Physical Activity andMortality in CKD
(NHANES III)
Patients followed for 7 years
• 15% of sample inactive
• 43% of sample insufficiently active
• 42% of sample met recommended levels of PA
19.
Exercise Capacity asa Predictor of Survival Among Ambulatory Patients with End-stage
Renal Disease
20.
The Bottom Line
•CKD is associated with reduced PA
• LTPA is associated with decreased
mortality in CKD
• VO2peak is a strong predictor of
survival
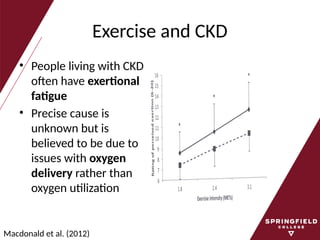
Exercise and CKD
•People living with CKD
often have exertional
fatigue
• Precise cause is
unknown but is
believed to be due to
issues with oxygen
delivery rather than
oxygen utilization
Macdonald et al. (2012)
23.
Exercise and CKD
•People with CKD have been shown to have
peak oxygen uptake values that average 50-
80% of normal age matched controls
• Limited data available on the effect of exercise
for patients living with predialysis
• Studies have shown improvements in oxygen
uptake similar to those living with ESRD
Johansen & Painter (2012)
29.
The Bottom Line
•Exercise training does NOT worsen kidney
function in CKD patients
• Resistance exercise improves muscle mass,
physical function and counteracts catabolism
of low protein diets and uremia with renal
failure
Exercise and theProgression of CKD
• Kidney function normally declines at the rate
of 1 mL/min/year
• In those with CKD, secondary to diabetes, the
rate of decline can exceed 10mL/min/year
• It has been well established that good blood
pressure control in addition to the use of ACE
inhibitors reduces the rate of decline
Jaber & Madias (2005)
32.
Exercise and theProgression of CKD
• There is some evidence from animal studies
that exercise training can modify kidney
function in CKD
• There have been a few published studies
with mixed results involving humans that
have investigated the impact of exercise
training on the progression of CKD
42.
The Bottom Line
•Aerobic exercise training appears to improve
VO2peak and heart rate values in predialysis
patients
• Higher amounts of habitual physical activity
associate with a slower GFR decline among
patients with CKD
Prevalence of CKD
•Researchers have noted that there are > 16
million stage 3 or 4 CKD patients
• But only ~ 400,000 dialysis patients
• Why is there this big gap between the
numbers of CKD patients in stage 3 or 4 of the
disease and those who “progress” to ESRD?
Beddhu et al. (2009)
45.
CKD and CVD
•Most CKD patients do NOT progress from
earlier stages of the disease to ESRD; rather,
most die prematurely of CVD
• Believed to be due to the presence of
traditional CVD risk factors and other risk
factors
– Traditional: HTN, dyslipidemia, diabetes
– Other: endothelial dysfunction, SNS activity,
oxidative stress, inflammation
Johansen & Painter (2011)
46.
CKD and ArterialStiffness
• Clear evidence demonstrates that people with
CKD have stiffer arteries, linked to:
– LVH
– CHF
– Strokes
– MI
• Arterial stiffness is considered an
independent risk factor for CVD
Greenwald (2007), Maeda et al. (2005), Otsuki et al. (2007)
47.
Exercise and ArterialStiffness
• Numerous researchers have reported aerobic
exercise to beneficially reduce arterial stiffness
in clinical and non-clinical populations
• However, no one has ever investigated the
effect or aerobic exercise on arterial stiffness
in a group of CKD patients
CKD and PhysicalFunction
• People living with CKD demonstrate marked impairment
in aerobic capacity, physical function, and lower habitual
levels of physical activity compared to healthy controls
• People with CKD and ESRD therefore exhibit higher rates
of
– Lower extremity dysfunction
– Sarcopenia
– Slower gait speed
– Physical inactivity
– Higher rates of fatigue and exhaustion
Weiner & Seliger (2014)
54.
The Bottom Line
•Medically stable patients living with CKD and
ESRD should be encouraged to participate in
moderately intense resistance exercise
– It is safe
– It can lead to substantial improvements in
function
Headley et al. (2012)
Conclusions
• CKD isa major and costly public health issue in the US
• Aerobic and resistance exercise may be used as a non-
pharmacological lifestyle therapy to treat and control
CKD
• Exercise does not worse kidney function and improves
cardiorespiratory, muscular, and functional parameters
of health
• Because exercise has been deemed to be both safe
and efficacious, the routine prescription of exercise
should be made to those living with CKD
References
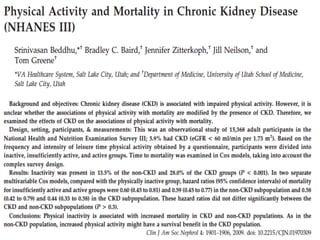
• Beddhu, S.,Baird, B. C., Zitterkoph, J., Neilson, J., & Greene, T. (2009). Physical activity and mortality in
chronic kidney disease (NHANES III). Clinical journal of the American Society of Nephrology : CJASN,
4(12), 1901–1906. doi:10.2215/CJN.01970309
• Boyce, M. L., Robergs, R. A., Avasthi, P. S., Roldan, C., Foster, A., Montner, P., … Nelson, C. (1997).
Exercise training by individuals with predialysis renal failure: cardiorespiratory endurance, hypertension,
and renal function. American Journal Of Kidney Diseases: The Official Journal Of The National Kidney
Foundation, 30(2), 180–192. Retrieved from
http://ezproxy.spfldcol.edu/login?url=http://search.ebscohost.com/login.aspx?
direct=true&db=cmedm&AN=9261028&loginpage=login.asp&site=ehost-live
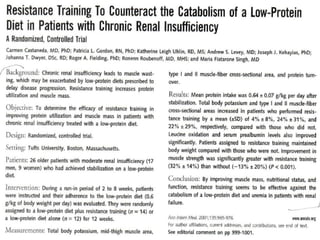
• Castandeda, C., Gordon, P. L., Uhlin, K. L., Levey, A. S., Kehayias, J. J., Dwyer, J. T., … Singh, M. F. (2001).
Resistance training to counteract the catabolism of a low-protein diet in patients with chronic renal
insufficiency. Ann Intern Med, 135(11), 965–976.
• Diesel, W., Noakes, T. D., Swanepoel, C., & Lambert, M. (1990). Isokinetic muscle strength predicts
maximum exercise tolerance in renal patients on chronic hemodialysis. American Journal Of Kidney
Diseases: The Official Journal Of The National Kidney Foundation, 16(2 (Print)), 109–114. Retrieved from
http://ezproxy.spfldcol.edu/login?url=http://search.epnet.com/login.aspx?
direct=true&db=cmedm&an=2382645&loginpage=login.asp
• Eidemak, I., Haaber, A. B., Feldt-Rasmussen, B., Kanstrup, I.-L., & Strandgaard, S. (1997). Exercise
Training and the Progession of Chronic Renal Failure. Nephron, 75, 36–40.
60.
References
• Greenwald, S.E. (2007). Ageing of the conduit arteries. Journal of Pathology, 211, 157–
172.
• Hayashi, K., Sugawara, J., Komine, H., Maeda, S., & Yokoi, T. (2005). Effects of aerobic
exercise training on stiffness of central and periperal arteries in middle-aged sedentary
men. Japanes Journal of Physiology, 55, 235–239.
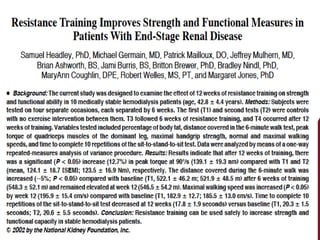
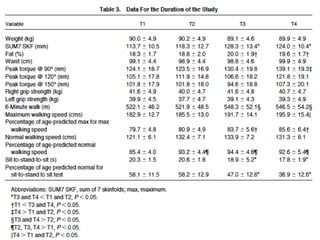
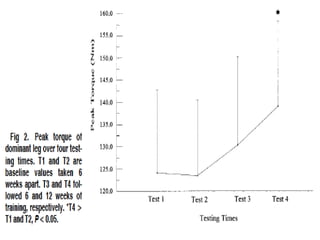
• Headley, S, Germain, M., Mailloux, P., Mulhern, J., Ashworth, B., Burris, J., … Nindl
Coughlin,M.,Welles,R.,Jones,M., B. (2002). Resistance training improves stgrength and
functional measures in patients with end-stage renal disease. Am J. Kidney Dis, 40(2),
355–364.
• Headley, Samuel, Germain, M., Milch, C., Pescatello, L., Coughlin, M. A., Nindl, B. C., …
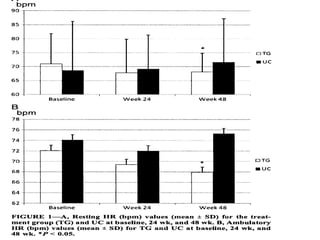
Wood, R. (2012). Exercise training improves HR responses and V˙O2peak in predialysis
kidney patients. Medicine and science in sports and exercise, 44(12), 2392–9.
doi:10.1249/MSS.0b013e318268c70c
• Heifets, M., Davis, T. A., Tegtmeyer, E., & Klahr, S. (1987). Exercise Training ameliorates
progressive renal disase in rats with subtotal nephrectomy. Kidney International, 32,
815–816,817,818,819,820.
61.
References
• Jaber, B.L., & Madias, N. E. (2005). Progression of chronic kidney disease: can it be
prevented or arrested? The American Journal of Medicine, 118(12), 1323–1330. Retrieved
from http://ezproxy.spfldcol.edu/login?url=http://search.ebscohost.com/login.aspx?
direct=true&db=cmedm&AN=16378772&loginpage=login.asp&site=ehost-live
• Johansen, K. L., & Painter, P. (2012). Exercise in individuals with CKD. American journal of
kidney diseases : the official journal of the National Kidney Foundation, 59(1), 126–34.
doi:10.1053/j.ajkd.2011.10.008
• Levey, A. S., & Stevens, L. A. (2010). Estimating GFR using the CKD Epidemiology
Collaboration (CKD-EPI) creatinine equation: more accurate GFR estimates, lower CKD
prevalence estimates, and better risk predictions. American Journal Of Kidney Diseases:
The Official Journal Of The National Kidney Foundation, 55(4), 622–627. Retrieved from
http://ezproxy.spfldcol.edu/login?url=http://search.ebscohost.com/login.aspx?
direct=true&db=mnh&AN=20338463&site=ehost-live
• Macdonald, J. H., Fearn, L., Jibani, M., & Marcora, S. M. (2012). Exertional fatigue in
patients with CKD. American journal of kidney diseases : the official journal of the National
Kidney Foundation, 60(6), 930–9. doi:10.1053/j.ajkd.2012.06.021
Editor's Notes
#5 National Kidney Foundation Kidney Disease Outcomes Quality Initiatives.
#9 Albumin is a water soluble protein
Creatinine formed from the breakdown of creatinine phosphate.
#14 Medicare provides health insurance for Americans aged 65 and older who have worked and paid into the system.
#18 Beddhu et al. reported on data from 15,368 individuals in NHANES III (1988-94).
A home interview was administered to the participants in this study.
Individuals were questioned about the frequency of LTPA within the previous month to estimate MET level
Based upon the results of the survey, individuals were divided into inactive (no LTPA), insufficiently active, active (3-6 METS, 5x/wk or >6 METS 3 or >/wk).
“..there is a considerable body of evidence that CKD is associated with poor functional status, and aerobic or resistance training can improve functional status in this population. However, there is a dearth of studies on the effects of physical activity on survival in the CKD population.”
#19 Survival status was determined for 175 patients living with ESRD for 3.5 years
VO2peak and other clinical data was obtained
23 deaths during the 3.5 year follow up period
VO2peak > 17.5 mL/min/kg was found to be a strong predictor of survivors
#22 Recent reports indicate a greater reliance on anaerobic metabolism (increased RER and lactate) in CKD patients to perform the same work.
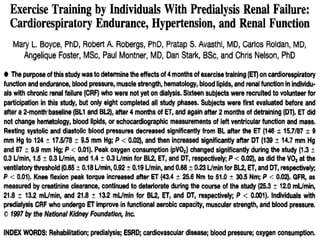
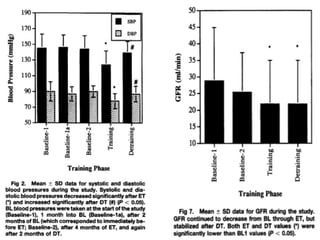
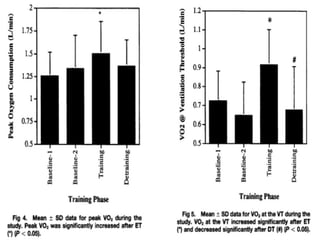
#24 “..investigate the effects of supervised exercise training (ET) on cardio respiratory endurance, cardiac performance, muscular strength, hematology, blood pressure, blood lipids, and renal function in predialysis chronic renal failure.”
Sixteen subjects were recruited for the study but only eight completed all aspects of the study.
Subjects were tested at baseline (2 times 2 months apart) then following 4 months of endurance training, then following 2 months of detraining.
The training program involved 3 supervised exercise sessions per week at an initial intensity of 50-60% heart rate reserve.
The duration of each session was gradually increased to 60 minutes (30 min walking, 30 min cycling).
This training program led to a 12% increase in peak oxygen uptake accompanied with an increase in the ventilatory threshold.
There was also a significant reduction in both systolic and diastolic pressures.
These all approached baseline values after the 2 month detraining period.
There were no changes in blood lipids (TC, HDL, LDL,TG), hematology variables (i.e.,Hhb or hct), or LV function (LVmass,LVEDV, LVESV).
“ET did not appear to further compromise renal function as the rate of decline in GFR appeared to be constant through the study period.”
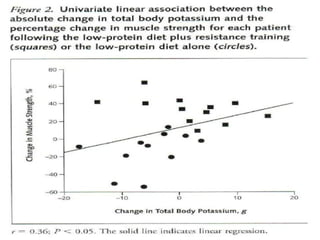
#28 Castaneda et al. (2001) demonstrated that a resistance training program resulted in a substantial benefit to pre-dialysis CKD patients who were on a low protein(0.6 g/kg body wt/day) diet.
Subjects trained 3 X week with 3 sets of 8 reps at 80% 1RM using 5 exercises (Chest & leg press; Latissimus pull-down; Knee extension & knee flexion)
The control group had a period of “sham exercise”.
The following increased in the treatment group: Muscular strength (32% vs -13%), Total body potassium (4%), Type 1 and type 2 muscle fiber cross sectional area (24%).
#32 Heifets et al. (1987) took six-week old Sprague-Dawley rats and had 75% of renal mass removed.
The rats were then randomly assigned to either the exercise training group (n=41) or to the control group (n=37).
The rats in the exercise group, swam for 2 hours daily while the rats in the control group did not.
After 2 months of training a number of variables were assessed in the rats including GFR, plasma creatinine, urine protein, plasma lipids (TC, LDL,TG). At the completion of the study the researchers found that exercise training led to:Improved GFR proteinuria evidence of glomerulosclerosis lipids (particularly LDL) bodyweight despite similar nutrient intakes!!
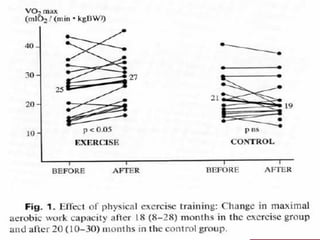
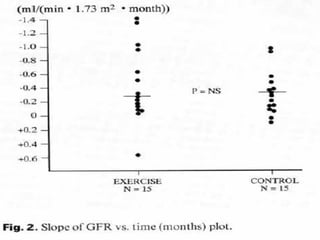
#35 Eidemak et al. (1997) took 30 non-diabetic CKD patients (GFR = 10-43 ml/min) and randomly assigned them to either the exercise group or to the control group.
Individuals in the exercise group were expected to exercise at home for 30 min daily at an intensity of 60-75% of maximal exercise capacity and they were to aim to expend 2,000 kcal/week.
Those in the control group were sedentary
Patients participated in the program for approximately 20 months.
At the end of the study the researchers found: VO2peak(ml/kg/min) 25 to 27 vs 21 to 19 (C) TC (mmol/l)in the exercise group 4.99±0.89 Pre vs 5.65±1.05 Post (E) 5.33±1.07 Pre vs 5.42±1.17 Post (C)
No difference in the rate of GFR decline between the groups:-0.28ml/min/month (C) -0.27ml/min/month (E)
“regular exercise does not have an untoward effect on progression of renal disease, despite repetitive exercise-related falls in renal blood flow, transiently increased proteinuria….”
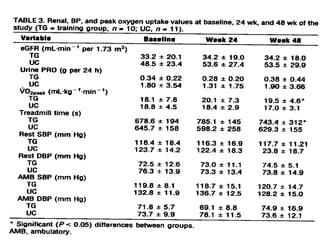
#38 “… the current pilot study was designed to determine the effects of long-term supervised exercise training and modest dietary modification on kidney function and indices of cardiovascular function in a sample of stage 2–4 CKD patients compared with a control group who received the current standard medical care”
Patients were matched for eGFR and VO2max
Then randomly assigned to either the intervention or control group.
Patients in the training group worked with a personal trainer 3 times per week for 48 weeks.
Aerobic training alone for the first 24 weeks
Combination of aerobic and resistance training during the last 24 weeks.
The rate of change in eGFR was not different between groups (TG = 0.071 ml/min/month; UC = 0.45 ml/min month; p = .39).
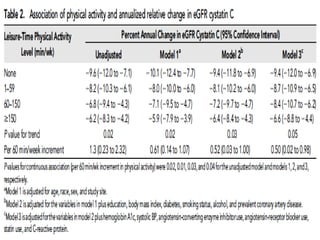
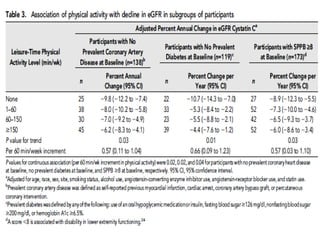
#41 Recently, Robinson-Cohen et al. (2014) demonstrated that a greater amount of leisure time physical activity was associated with a slower rate of eGFR decline in stage 3-4 CKD patients.
“Specifically, we found a 2.8% difference in annual eGFR decline comparing the highest to lowest category of physical activity after adjustment for sociodemographic factors and prevalent diseases.”
Metabolic consequences of CKD include:Insulin resistance, Dyslipidemia, Sodium retention, Accumulation of small molecular toxins
#47 Hayashi et al. (2005) aerobically trained 17 sedentary normotensive middle-aged men for 16 weeks.
They measured both central (carotid-femoral)and peripheral arterial stiffness using applanation tonometry.
They also measured the compliance in these arteries using ultrasound.
They found that the 16 weeks of aerobic training led to a reduction of central arterial stiffness but not peripheral stiffness.
Edwards et al. (2004) found that 12 weeks of aerobic training in a cardiac rehab program led to a significant reduction in arterial stiffness as measured by the augmentation index.
Ferrier et al (2001), however found that a 8 weeks of aerobic training did not alter central arterial stiffness values in a group patients who had isolated systolic hypertension.
Collier et al. (2008) found that 4 weeks of either aerobic or resistance training had contrasting effects on arterial stiffness in a group of pre-hypertensive or stage 1 hypertensive non-mediated individuals.
Aerobic training led to a reduction in both central and peripheral arterial stiffness while resistance training led to an increase.
#53 Ten medically stable hemodialysis patients volunteered to participate in the study.
Age (yrs) 42.8 ± 4.4
HD duration (m)41.6 ± 19
Gender 7 (M) 3 (F)
Race 4 (B) 6 (W)
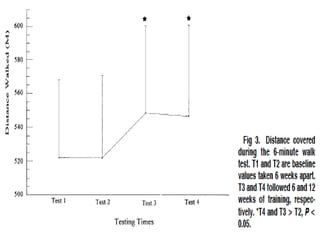
Each subject was tested on four separate occasions, each 6 weeks apart.
During each testing session the following were measured:Body composition (skinfolds), 6-min walk test, Peak torque of quadriceps (dominant leg) (Cybex), Grip test, Gait speed test (20 ft distance), Sit-to-stand-to-sit test (time to complete 10 cycles)
Subjects initially used 1 set of 10-15 reps of 9 exercises.
When subjects were able to complete 15 repetitions with an RPE of 10-12 (fairly light), the weight was gradually increased.
By the completion of the study, subjects were performing 2-3 sets of each exercise.







![PHYSICAL EXERCISE koreksi [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/physicalexercisekoreksiautosaved-250612131516-8ce43ae6-thumbnail.jpg?width=640&height=640&fit=bounds)














































