Downloaded 14 times
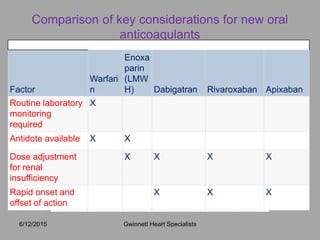
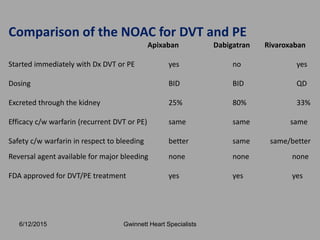
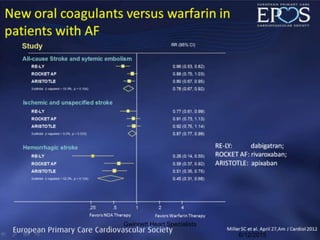
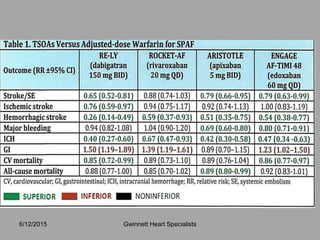
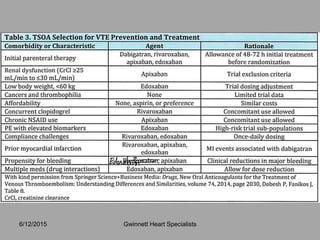
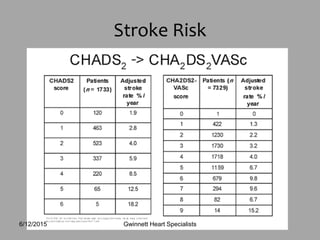
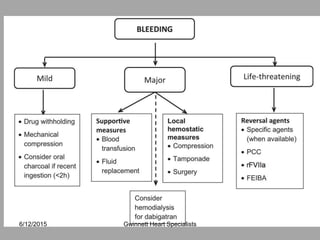

Sreeni Gangasani is a cardiologist who specializes in general cardiology, echocardiography, nuclear cardiology, and preventive cardiology. He received his medical degree and residency training in India and completed fellowship training at William Beaumont Hospital. The document discusses newer oral anticoagulants (NOACs) including dabigatran, rivaroxaban, apixaban, and edoxaban which are alternatives to warfarin for treating and preventing blood clots. It provides details on their mechanisms of action, pharmacokinetics, FDA-approved indications, and practical considerations for use.










































































