This study characterized patients on direct oral anticoagulants (DOACs) undergoing elective coronary procedures and examined adherence to guidelines for interrupting DOACs before the procedures. The study found that physician adherence to the health center's guideline was low at 12.5%, and that patient adherence to instructions was 70.8%. While longer interruptions of DOACs did not significantly lower drug levels, traditional coagulation tests did not correlate with DOAC levels. Barriers to the guideline's use included a lack of agreement on bleeding risk and unclear holding instructions. The study aims to update guidelines to improve safety in peri-procedural DOAC management.
Feasibility Solutions to Clinical Trial Nightmaresjbarag
Slow patient recruitment and poor retention cause recurrent nightmares and perpetual problems often resulting in missing recruitment milestones. The cost of these delays represents hundreds of thousands of dollars for drug and device developers. By recognizing this issue, early detailed feasibility can provide planning and contingency solutions that are focused on reducing the impact of delayed recruitment. Furthermore understanding what motivates investigators and patients to actively participate in clinical studies and how patient recruitment strategies and materials can support all stakeholders to complete studies on time are critical aspects of clinical study delivery planning.
During this presentation, an experienced Premier Research feasibility and patient recruitment specialist, reviewed feasibility approaches to address protocol evaluation as well as addressed influences on country selection, site distribution and patient recruitment strategies to provide for more effective clinical trial planning and conduct.
For more information, go to http://www.premier-research.com.
EVIDENCE-BASED CPGs FOR HEMATOLOGY - ONCOLOGY UNIT, KING SAUD UNIVERSITY HOPSITALS
Saudi Arabia, Riyadh
King Saud University Hospitals
CPGs Committee
Quality Management Dept
CPGs Program
By YASSER SAMI AMER
Feasibility Solutions to Clinical Trial Nightmaresjbarag
Slow patient recruitment and poor retention cause recurrent nightmares and perpetual problems often resulting in missing recruitment milestones. The cost of these delays represents hundreds of thousands of dollars for drug and device developers. By recognizing this issue, early detailed feasibility can provide planning and contingency solutions that are focused on reducing the impact of delayed recruitment. Furthermore understanding what motivates investigators and patients to actively participate in clinical studies and how patient recruitment strategies and materials can support all stakeholders to complete studies on time are critical aspects of clinical study delivery planning.
During this presentation, an experienced Premier Research feasibility and patient recruitment specialist, reviewed feasibility approaches to address protocol evaluation as well as addressed influences on country selection, site distribution and patient recruitment strategies to provide for more effective clinical trial planning and conduct.
For more information, go to http://www.premier-research.com.
EVIDENCE-BASED CPGs FOR HEMATOLOGY - ONCOLOGY UNIT, KING SAUD UNIVERSITY HOPSITALS
Saudi Arabia, Riyadh
King Saud University Hospitals
CPGs Committee
Quality Management Dept
CPGs Program
By YASSER SAMI AMER
Principles of Surgical Audit presented by Meeran Earfan, Kurdistan Board Trainee/General Surgery in Sulaimaniyah Teaching Hospital, As Sulaimaniyah, Iraq
Providing a course that is relevant, practical and patient-centered that will positively impact the speed in which entry-level oncology specialists integrate into the oncology practice setting.
Improving Lab Order, Verification, and Follow-up Processes at UT PhysiciansAllison McCoy
We retrieved electronic health record data on lab order, verification, and follow-up processes at UT Physicians and developed a dashboard to describe metrics for evaluating these processes. A two-month pilot evaluation of one department indicates some room for improvement in standardizing and improving processes to improve quality of care, patient safety, and satisfaction.
Introduction of the NZ Health IT Plan enables better gout management - Reflections of an early adopter. Presented by Peter Gow, Counties Manukau DHB, at HINZ 2014, 12 November 2014, 11.37am, Plenary Room
The shared radiology workflow consists of physician’s referral, study approval, scheduling, patient arrival, imaging, reporting, validating, and results distribution. The performance of this process can be measured on different levels: resources utilization, current operations, and outcomes.
The end-result of the process is defined by the goal, which can also vary. The major goals are effectiveness (e.g. high-quality, high-safety, high-volume, high-accessibility services, patients’ and physicians’ satisfaction), efficiency (cost-effectiveness, cost-control, revenue generation), and health improvement (better treatment because of accurate diagnostics, less morbidity and mortality because of early diagnostics).
The problem with the radiology services is that we often incorrectly measure incorrect metrics. Wherever we see systematic measurement of results in health care—no matter what the country—we see those results improve (R.S. Kaplan, M.E. Porter).
Hence, we should move from current radiology operational metrics (report turn-around-time, back-log time, discrepancies, equipment utilization rate, revenue) to clinical operational metrics (diagnosis-related delays of treatment, time to begin treatment) and outcome measurements (patients’ and clinicians’ satisfaction, gross margin of services, involvement in disease-specific clinical teams, better treatment because of accurate diagnostics).
The best method for tackling ‘bottlenecks’ is time-driven activity-based costing (TDABC) through better resource utilization, standardized processes, proper staffing, and logistics optimization.
Building an enabling IT platform is the key for embedding the changes in the system.
Ideal physician measurements are aligned to electronic data collection, attributable to individuals, cascade from organizational goals, supported by evidence and physicians, comparative, and transparent.
This presentation has the measures to be taken for the safety of patients. It covers the 6 goals
Goal 1: Identify patients correctly
Goal 2: Improve effective communication
Goal 3: Improve the safety of high-alert medications
Goal 4: Ensure safe surgery
Goal 5: Reduce the risk of health care-associated infections
Goal 6: Reduce the risk of patient harm resulting from falls
Patient Blood Management: Impact of Quality Data on Patient OutcomesViewics
Patient blood management (PBM) has been proven to improve patient outcomes and save hospitals millions of dollars. Ensuring the quality of your data is central to decision making and critical to having a strong PBM program.
Would you like to learn how your organization can improve patient outcomes by implementing a PBM program based on accurate data?
If so, view this presentation by blood management expert Lance Trewhella. Lance presents how to develop a successful, evidence-based, multidisciplinary PBM program aimed at optimizing the care of patients who might need transfusion.
You’ll learn:
• Current recommendations for blood transfusion utilization
• The impact of quality data on PBM programs
• Best data practices in PBM
Principles of Surgical Audit presented by Meeran Earfan, Kurdistan Board Trainee/General Surgery in Sulaimaniyah Teaching Hospital, As Sulaimaniyah, Iraq
Providing a course that is relevant, practical and patient-centered that will positively impact the speed in which entry-level oncology specialists integrate into the oncology practice setting.
Improving Lab Order, Verification, and Follow-up Processes at UT PhysiciansAllison McCoy
We retrieved electronic health record data on lab order, verification, and follow-up processes at UT Physicians and developed a dashboard to describe metrics for evaluating these processes. A two-month pilot evaluation of one department indicates some room for improvement in standardizing and improving processes to improve quality of care, patient safety, and satisfaction.
Introduction of the NZ Health IT Plan enables better gout management - Reflections of an early adopter. Presented by Peter Gow, Counties Manukau DHB, at HINZ 2014, 12 November 2014, 11.37am, Plenary Room
The shared radiology workflow consists of physician’s referral, study approval, scheduling, patient arrival, imaging, reporting, validating, and results distribution. The performance of this process can be measured on different levels: resources utilization, current operations, and outcomes.
The end-result of the process is defined by the goal, which can also vary. The major goals are effectiveness (e.g. high-quality, high-safety, high-volume, high-accessibility services, patients’ and physicians’ satisfaction), efficiency (cost-effectiveness, cost-control, revenue generation), and health improvement (better treatment because of accurate diagnostics, less morbidity and mortality because of early diagnostics).
The problem with the radiology services is that we often incorrectly measure incorrect metrics. Wherever we see systematic measurement of results in health care—no matter what the country—we see those results improve (R.S. Kaplan, M.E. Porter).
Hence, we should move from current radiology operational metrics (report turn-around-time, back-log time, discrepancies, equipment utilization rate, revenue) to clinical operational metrics (diagnosis-related delays of treatment, time to begin treatment) and outcome measurements (patients’ and clinicians’ satisfaction, gross margin of services, involvement in disease-specific clinical teams, better treatment because of accurate diagnostics).
The best method for tackling ‘bottlenecks’ is time-driven activity-based costing (TDABC) through better resource utilization, standardized processes, proper staffing, and logistics optimization.
Building an enabling IT platform is the key for embedding the changes in the system.
Ideal physician measurements are aligned to electronic data collection, attributable to individuals, cascade from organizational goals, supported by evidence and physicians, comparative, and transparent.
This presentation has the measures to be taken for the safety of patients. It covers the 6 goals
Goal 1: Identify patients correctly
Goal 2: Improve effective communication
Goal 3: Improve the safety of high-alert medications
Goal 4: Ensure safe surgery
Goal 5: Reduce the risk of health care-associated infections
Goal 6: Reduce the risk of patient harm resulting from falls
Patient Blood Management: Impact of Quality Data on Patient OutcomesViewics
Patient blood management (PBM) has been proven to improve patient outcomes and save hospitals millions of dollars. Ensuring the quality of your data is central to decision making and critical to having a strong PBM program.
Would you like to learn how your organization can improve patient outcomes by implementing a PBM program based on accurate data?
If so, view this presentation by blood management expert Lance Trewhella. Lance presents how to develop a successful, evidence-based, multidisciplinary PBM program aimed at optimizing the care of patients who might need transfusion.
You’ll learn:
• Current recommendations for blood transfusion utilization
• The impact of quality data on PBM programs
• Best data practices in PBM
Evaluating the impact of a specialist frailty multidisciplinary team pathway ...Health Innovation Wessex
The Health Innovation Network Polypharmacy Programme is working with healthcare professionals to address problematic polypharmacy by supporting easier identification of patients at potential risk from harm from multiple medications.
Our evidence-based polypharmacy Action Learning Sets (ALS) are being rolled out across England to support GPs, pharmacists and other healthcare professionals who undertake prescribing or medication reviews to understand the complex issues around stopping inappropriate medicines safely.
To drive and accelerate changes in practice, delegates complete a quality improvement project to address problematic polypharmacy in their workplace. This poster summary, Evaluating the impact of a specialist frailty multidisciplinary team pathway with clinical pharmacist involvement, can be viewed here.
For more information about the polypharmacy programme, please visit https://thehealthinnovationnetwork.co.uk/programmes/medicines/polypharmacy/
Clinical practice guidelines are “systematically developed statements to assist practitioner and patient decisions about appropriate health care for specific clinical circumstances.”They are intended to offer concise instructions on how to provide healthcare services.The most important benefit of clinical practice guidelines is their potential to improve both the quality or process of care and patient outcomes. Increasingly, clinicians and clinical managers must choose from numerous, sometimes differing, and occasionally contradictory, guidelines.
Its a power point presentation on evidence based dentistry and its application in branch of Prosthodontics, thus named as Evidence based Prosthodontics.
Rapid review of current service provision following cancer treatmentNHS Improvement
NHS Improvement carried out a rapid review of current provision of services for breast, prostate and colorectal cancer patients following treatment during the summer of 2009 at the request of the National Cancer Survivorship Initiative (NCSI). This publication shares the findings from this review.
(Published September 2010)
A review of the total knee replacement pathway: Integrated care is quality careApollo Hospitals
A Total Knee Replacement (TKR) Pathway (adapted from the Credit Valley Hospital, Canada) is in place at the Apollo Health city facility since 2011. We re-visited the pathway design and the priority grid that led to its adaptation. We analyzed the data with the aim to analyze repetitive and unique trends and evaluate the performance of the pathway. Even with the increased volume the patient satisfaction rose from 56% at the time of pathway implementation to 77% at the end of the evaluation period of 45 months. The Average Length of Stay reduced by 27% from 7.94 to 5.78 days (the difference between the initial and final recorded values), in the same evaluation time period. The methodology of evaluation of the pathway was adapted from the Leuven Clinical Pathway Compass 5 way approach.
1
Quantitative Synopsis and Appraisal
Studentfirstname Studentlastname
College of Nursing, Resurrection University
NUR4440: Research in Nursing
Professor Carina Piccinini
February 14, 2020
2
Quantitative Appraisal and Synopsis
The purpose of this paper is to summarize and appraise a research study testing the use of
disinfectant caps on intravenous (IV lines) to reduce the rate of hospital associated bloodstream
infections (BSI). The Centers for Disease Control and Prevention (CDC, 2019) reports that
central line associated bloodstream infections (CLABSI) remain a major concern in hospital
settings causing fatalities, increased length of stay, and increased costs. The CDC (2019)
recommends proper maintenance of intravenous lines to reduce the risk of infection. Current
research is still looking to define what proper maintenance should be, including whether
disinfectant caps influence rates of infection for intravenous (IV) lines.
Summary of the Study
The CDC recommends that healthcare workers disinfect all needleless connectors for
peripheral and central IVs prior to connection to reduce the risk of CLABSIs without further
recommendation on the type or length of disinfections. The authors of this study note other
studies have tested disinfecting caps and sought to confirm those results.
Merrill et al. (2014) conducted a quasi-experimental study to identify if disinfectant caps
reduce CLABSI incidence and the relationship between nursing compliance with the caps and
CLABSI rates. This study was held in a single Trauma 1 hospital with 430 beds in the United
States.
The researchers obtained their sample through nonrandom convenience sampling by
including all patients meeting inclusion criteria at the hospital starting January 2012. Participants
were included if they had a central or peripheral intravenous line, of any age, and were admitted
to 13 specific hospital floors. Subjects were excluded if they were on the following floors:
emergency department; labor, delivery or post-partum; ambulatory care, surgical services; and
Commented [CP1]: This answers “Why is this important
to study?” It’s not just ensuring our patients do not get
CLABSIs…it goes beyond that to fatalities, length of stay in
hospitals, and healthcare costs.
The CDC and other healthcare related organizations are great
sources of information on the importance of topics.
Commented [CP2]: What is known (recommendation to
disinfect ports), not known (what specifically should be
used), and gap in knowledge (confirmation of other study
results).
This information is found in the introduction to every
research article. DO NOT use the discussion/conclusions
section of an article for this information! It will be
WRONG.
Commented [CP3]: Study being summarized/appraised is
correctly cited.
Specific research design stated.
Setting of study stated.
3
well-baby nursery. The study did ...
1 Quantitative Synopsis and Appraisal StudentfAbbyWhyte974
1
Quantitative Synopsis and Appraisal
Studentfirstname Studentlastname
College of Nursing, Resurrection University
NUR4440: Research in Nursing
Professor Carina Piccinini
February 14, 2020
2
Quantitative Appraisal and Synopsis
The purpose of this paper is to summarize and appraise a research study testing the use of
disinfectant caps on intravenous (IV lines) to reduce the rate of hospital associated bloodstream
infections (BSI). The Centers for Disease Control and Prevention (CDC, 2019) reports that
central line associated bloodstream infections (CLABSI) remain a major concern in hospital
settings causing fatalities, increased length of stay, and increased costs. The CDC (2019)
recommends proper maintenance of intravenous lines to reduce the risk of infection. Current
research is still looking to define what proper maintenance should be, including whether
disinfectant caps influence rates of infection for intravenous (IV) lines.
Summary of the Study
The CDC recommends that healthcare workers disinfect all needleless connectors for
peripheral and central IVs prior to connection to reduce the risk of CLABSIs without further
recommendation on the type or length of disinfections. The authors of this study note other
studies have tested disinfecting caps and sought to confirm those results.
Merrill et al. (2014) conducted a quasi-experimental study to identify if disinfectant caps
reduce CLABSI incidence and the relationship between nursing compliance with the caps and
CLABSI rates. This study was held in a single Trauma 1 hospital with 430 beds in the United
States.
The researchers obtained their sample through nonrandom convenience sampling by
including all patients meeting inclusion criteria at the hospital starting January 2012. Participants
were included if they had a central or peripheral intravenous line, of any age, and were admitted
to 13 specific hospital floors. Subjects were excluded if they were on the following floors:
emergency department; labor, delivery or post-partum; ambulatory care, surgical services; and
Commented [CP1]: This answers “Why is this important
to study?” It’s not just ensuring our patients do not get
CLABSIs…it goes beyond that to fatalities, length of stay in
hospitals, and healthcare costs.
The CDC and other healthcare related organizations are great
sources of information on the importance of topics.
Commented [CP2]: What is known (recommendation to
disinfect ports), not known (what specifically should be
used), and gap in knowledge (confirmation of other study
results).
This information is found in the introduction to every
research article. DO NOT use the discussion/conclusions
section of an article for this information! It will be
WRONG.
Commented [CP3]: Study being summarized/appraised is
correctly cited.
Specific research design stated.
Setting of study stated.
3
well-baby nursery. The study did ...
1. Background
Objectives
Methods
Results
Discussion and Implications
•The use of direct oral anticoagulants (DOACs) is increasing and there is a greater need
to understand how to manage DOACs in specific clinical scenarios (e.g. patients who
require interruption for procedures) in order to optimize safety.
• At Sunnybrook Health Sciences Centre (SHSC), there is a guideline for peri‐procedural
management of DOACs on the intranet, but we are unaware of how often this guideline
is used in practice and how clinicians make their decisions peri‐procedurally.
•This study was conducted to identify the gap between the guideline and practice and
to characterize patients’ adherence to instructions for peri‐procedural management of
anticoagulants.
1. Characterize the patient population receiving DOACs and undergoing elective
coronary angiography.
2. Examine current peri‐procedural practices at SHSC and the associated outcomes
a) Physician adherence to SHSC Guideline
b) Patient adherence to physicians’ instructions
3. Examine patients’ pre‐procedural coagulation levels (by obtaining a pre‐
procedural blood sample) and describe any relationships with the outcomes
4. Make recommendations to update and improve existing guidelines for peri‐
procedural management of DOACs
This is a prospective, observational study conducted in patients who were receiving
DOACs and undergoing elective coronary angiography (CA) with our without subsequent
percutaneous coronary intervention (PCI).
Eligible
Patient
1. Informed Consent Letter
2. Patient Information Collected
3. Physician Instructions to
Patients Collected
4. Blood sample collected
Pre‐procedure
Post‐procedure
•Informal interviews were conducted with cardiac triage coordinators who are responsible
for booking procedure appointments and relaying physicians’ instructions to patients to
identify current practice and practice use of the guideline.
•A brief informal questionnaire was distributed to physicians to understand how peri‐
procedural decisions regarding DOAC management were made.
•Anti‐Xa levels were measured for apixaban and rivaroxaban using the HemoSIL® and
Biophen® DiXal assays respectively. Dilute thrombin time (Hemoclot®) was used to measure
dabigatran levels. PT, INR, PTT and Thrombin Time were also run on all the samples.
•Descriptive statistics was used to analyze the data.
Peri‐procedural Info Collected
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
1 3 5 7 9 11 13 15 17 19 21 23
# of Days
DOACs Held
Patient Number
Patient Adherence to Physician Instructions
Physician
Instruction
s
Number of
Days the
Patient
Held DOAC
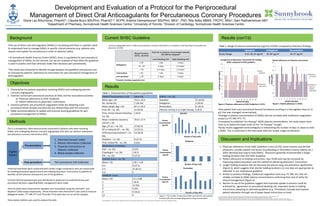
Figure 2. Physician adherence to SHSC Guideline is 12.5%. Figure 3. Patient adherence is 70.8%.
0
5
10
15
20
25
30
35
40
45
0 1.5 2 2 2 3 3 3 3 3 4
Plasma
Concentration
(ng/ml)
Number of Days Held
Apixaban
0
5
10
15
20
25
30
35
1 2 3 4 4
Plasma
Concentration
(ng/ml)
Number of Days Held
Dabigatran
0
5
10
15
20
25
30
35
40
0 1.5 2 2 2 3 3 3
Plasma
Concentration
(ng/ml)
Number of Days Held
Rivaroxaban
Apixaban Dabigatran Rivaroxaban
Study Range 0.41‐38.10 ng/ml 10‐30 ng/ml 16‐37 ng/ml
Figure 1. The number of days each DOAC was held for each patient
is shown with the corresponding plasma drug concentration.
Results (con’t’d)
Table 2. Range of plasma concentrations (ng/ml) of DOAC compared to literature findings.
1. Physician adherence to the SHSC Guideline is low (12.5%). Some reasons may be that
physicians consider patient risk factors (e.g bleeding or thrombotic history, elderly, etc.)
when deciding how long to hold DOACs. Physicians generally recommended a longer
holding duration than the SHSC Guideline.
2. Patient adherence to holding instructions was 70.8% and may be increased by
improving patient education and the method of delivering physicians’ instructions.
3. Longer holding durations did not decrease the plasma drug concentrations significantly
(Figure 3), which suggests that shorter holding durations (i.e one day) are appropriate as
reflected in our institutional guideline.
4. Similar to previous findings, traditional coagulation tests (e.g. PT, INR, etc.) did not
reliably correlate to DOAC plasma concentrations confirming their lack of utility for
clinical management (Figure 4).
5. Barriers to use of the guideline suggest that improved uptake in practice could be
achieved by: agreement on procedural bleeding risk, improved clarity in holding
instructions, adopting an alternate guideline (e.g. Thrombosis Canada) and improve
patient education through use of paper‐based instructions or tools.
Coronary angiography with or without percutaneous coronary intervention is considered a low bleeding risk procedure by
physicians at SHSC.
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
1 3 5 7 9 11 13 15 17 19 21 23
# of Days to Hold DOAC
Patient Number
Comparison of physicians' instructions for holding
DOAC compared to SHSC guideline
SHSC
Guideline
Physicians'
Instructions
Patient Characteristics n=24 Value (%)
Mean age ± SD 75.8 ± 10.4
No. female (%) 7 (29.2%)
Mean weight (kg) ± SD 87.4 ± 26.4
Prior MI – no. (%) 11 (45.8)
Prior clinical relevant bleeding –
no. (%)
2 (8.3)
Mean creatinine clearance
ml/min ± SD
70.8 ± 27.9
Age >75 yrs – no. (%) 15 (62.5)
HF or reduced LEF – no. (%) 13 (54.2)
HTN requiring treatment – no.
(%)
23 (95.8)
Diabetes – no. (%) 9 (37.5)
Prior stroke/TIA – no. (%) 6 (25)
Medications at Baseline
ASA – no. (%) 6 (25)
Clopidogrel – no. (%) 2 (8.3)
PPI – no. (%) 9 (37.5)
CHADS2 Score – no. (%)
Mean ± SD 2.96 ± 1.04
0‐2 9 (37.5)
3‐4 15 (62.5)
5‐6 0
HASBLED Score
Mean ± SD 2.5 ± 0.88
1 2 (8.3)
2 12 (50)
3 6 (25)
4 4 (16.6)
>5 0
DOACs – no. (%)
Apixaban 11 (45.8)
Dabigatran 5 (20.8)
Rivaroxaban 8 (33.3)
Patients coming in on triple therapy 2 (8.3) •One patient had a peri‐procedural femoral hematoma resulting in a hemoglobin drop of 12
g/L that was managed conservatively .
•Changes in plasma concentrations of DOACs did not correlate with traditional coagulation
assays (i.e PT, INR, PTT, TT)
•Compared to published “on‐therapy” DOAC plasma concentrations, the study values were
close to or below the lower limits of the “on‐therapy” troughs
•Study results suggested some ambiguity in interpreting the number of days vs. doses to hold
a DOAC. This is confirmed in the interviews with the cardiac triage coordinators.
1. Atul et al. 2014 focused update of the Canadian Cardiovascular Society Guidelines for the management of atrial fibrillation. Can J Cardiol. 2014;30:1114‐30.
2. Thrombosis Canada. Peri‐operative management of patients who are receiving new oral anticoagulant (dabigatran, rivaroxaban, apixaban).
3. Heidbuchel H et al. European Heart Rhythm Association practical guide on the use of new oral anticoagulants in patients with non‐valvular atrial fibrillation. Eurospace. 2013;15:626‐51.
4. Sunnybrook Health Sciences Center Thromboembolism Service. Peri‐Procedure management of patients receiving an oral direct inhibitor of coagulation (apixaban, rivaroxaban, dabigatran). 2014.
Table 1. Characteristics of the patient population.
Development and Evaluation of a Protocol for the Periprocedural
Management of Direct Oral Anticoagulants for Percutaneous Coronary Procedures
Gloria Lau BSc(Hons), PharmD1; Claudia Bucci BScPhm, PharmD1,2, ACPR; Artemis Diamantouros2 BScPhm, MEd1,, PhD; Rita Selby MBBS, FRCPC, MSc2; Sam Radhakrishnan MD3
1Department of Pharmacy, Sunnybrook Health Sciences Centre; 2University of Toronto; 3Division of Cardiology, Sunnybrook Health Sciences Centre
Current SHSC Guideline
Acknowledgements: Thank you to the coagulation laboratory at Sunnybrook Health Sciences Centre and St. Michael’s Hospital for performing the coagulation testing.