Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Does distance alone impact heart patients' healthcare access
Similar to Does distance alone impact heart patients' healthcare access (20)
Does distance alone impact heart patients' healthcare access
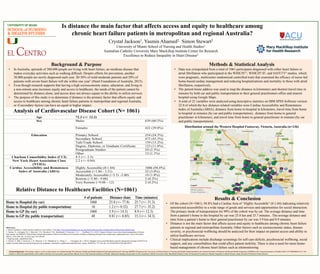
- 1. Is distance the main factor that affects access and equity to healthcare among chronic heart failure patients in metropolitan and regional Australia? Background & Purpose • In Australia, upwards of 300,000 people are living with heart failure, an insidious disease that makes everyday activities such as walking difficult. Despite efforts for prevention, another 30,000 people are newly diagnosed each year. 20-30% of mild-moderate patients and 50% of patients with severe heart failure will die within one year1 (Heart Foundation of Australia, 2015). • Even though research supports that having a high socioeconomic status, education, and living in a non-remote area increases equity and access to healthcare, the needs of the patient cannot be determined by distance alone, and access does not always equate to the ability to utilize services. • The purpose of this study is to determine if distance is the primary factor that affects equity and access to healthcare among chronic heart failure patients in metropolitan and regional Australia, or if secondary factors can have an equal or higher impact. Analysis of Cardiovascular Disease Cohort (N= 1061) Relative Distance to Healthcare Facilities (N=1061) Acknowledgements: The primary author’s work on this project was funded through The Minority Health and Health Disparities International Research Training (MHIRT) Program at the University of Miami School of Nursing and Health Studied funded by the National Institute of Minority Health and Health Disparities (NIMHD) at the National Institutes of Health (NIH) (1T37MD008647-01). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Additional funding was provided by the Australian Catholic University Mary Mackillop Institute Center for Research Excellence to Reduce Inequality in Heart Disease, under the lead of Professor Simon Stewart. Results & Conclusion • Of the cohort (N=1061), 94.8% had a Cardiac Aria of “Highly Accessbile” (0-1.84) indicating relatively unrestricted accessibility to a wide range of goods and services and opportunities for social interaction. The primary mode of transportation for 99% of the cohort was by car. The average distance and time from a patient’s home to the hospital by car was 25.8 km and 25.7 minutes.. The average distance and time from a patient’s home to their general practitioner by car was 5.9 km and 8.9 minutes. • Distance is not the main factor that affects access and equity to healthcare among chronic heart failure patients in regional and metropolitan Australia. Other factors such as socioeconomic status, disease severity, or psychosocial wellbeing should be analyzed for their impact on patient access and ability to utilize healthcare services. • Clinical implications include discharge screenings for self-care deficits, psychosocial wellbeing, social support, and any comorbidities that could affect patient mobility. There is also a need for more home- based management of chronic heart failure such as telemonitoring. Crystal Jackson1, Yasmin Ahamed2, Simon Stewart2 University of Miami School of Nursing and Health Studies1 Australian Catholic University Mary Mackillop Institute Center for Research Excellence to Reduce Inequality in Heart Disease2 Methods & Statistical Analysis • Data was extrapolated from a total of 1061 participants diagnosed with either heart failure or atrial fibrillation who participated in the WHICH? 2, WHICH? II3, and SAFETY4 studies, which were pragmatic, multicenter randomized controlled trials that examined the efficacy of nurse-led home-based cardiac management and reducing hospitalizations and mortality in those with atrial fibrillation, respectively. • The patient home address was used to map the distance in kilometers and shortest travel time in minutes by both car and public transportation to their general practitioners office and nearest hospital using Google Maps. • A total of 22 variables were analyzed using descriptive statistics on IBM SPSS Software version 22.0 of which the key distance-related variables were Cardiac Accessibility and Remoteness Index of Australia (ARIA), distance from home to hospital in kilometers, travel time from home to hospital in minutes (by car and public transportation), distance from home to general practitioner in kilometers, and travel time from home to general practitioner in minutes (by car and public transportation). Distribution around the Western Hospital Footscray, Victoria, Australia (n=136) Legend: Western Hospital Footscray Patient residence General Practitioner References: 1. Heart Foundation. Cardiovascular conditions, heart failure., from http://www.heartfoundation.org.au/your-heart/cardiovascular-conditions/Heart-failure/Pages/default.aspx 2. Stewart, S., Carrington, M. J., Marwick, T. H., Davidson, P. M., Macdonald, P., Horowitz, J. D., . . . Scuffham, P. A. (2012). Impact of home versus clinic-based management of chronic heart failure: the WHICH? (Which Heart Failure Intervention Is Most Cost-Effective & Consumer Friendly in Reducing Hospital Care) multicenter, randomized trial. J Am Coll Cardiol, 60(14), 1239-1248. doi: 10.1016/j.jacc.2012.06.025 3.Ongoing study, unpublished data 4. Stewart, S., Ball, J., Horowitz, J. D., Marwick, T. H., Mahadevan, G., Wong, C., . . . Carrington, M. J. (2015). Standard versus atrial fibrillation-specific management strategy (SAFETY) to reduce recurrent admission and prolong survival: pragmatic, multicentre, randomised controlled trial. Lancet, 385(9970), 775-784. doi: 10.1016/S0140-6736(14)61992-9 Age 72.3 (+/- 12.2) Sex Males 639 (60.2%) Females 422 (39.8%) Education Primary School 254 (24.3%) Secondary School 473 (45.3%) Tafe/Trade School 159 (15.2%) Degree, Diploma, or Graduate Certificate 123 (11.8%) Postgraduate Studies 24 (2.3%) Other 12 (1.1%) Charlson Comorbidity Index (CCI) 4.5 (+/- 2.5) New York Heart Association Class (NYHA) 2.2 (+/- 0.84) Cardiac Accessibility and Remoteness Index of Australia (ARIA) Highly Accessible (0-1.84) 1006 (94.8%) Accessible (>1.84 - 3.51) 32 (3.0%) Moderately Accessible (>3.51 -5.80) 19 (1.8%) Remote (>5.80 - 9.08) 2 (0.2%) Very Remote (>9.08 – 12) 2 (0.2%) # of patients Distance (km) Time (minutes) Home to Hospital (by car) 1060 25.8 (+/- 77.8) 25.7 (+/- 51.3) Home to Hospital (by public transportation) 16 1.2 (+/- 0.52) 27.7 (+/- 35.2) Home to GP (by car) 1060 5.9 (+/- 14.5) 8.9 (+/- 12.3) Home to GP (by public transportation) 48 0.81 (+/- 0.85) 15.3 (+/- 34.3)