3. 3
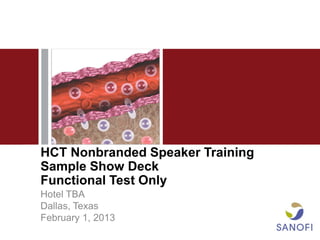
The Incidence of Myeloma Peaks in Patients
65 to 74 Years of Age
Age at Myeloma Diagnosis
30
25
Diagnoses, %
20
15
10
5
0
<20 20-34 35-44 45-54 55-64 65-74 75-84 ≥85
Age, years
Surveillance epidemiology and end results. SEER Stat Fact Sheets: Myeloma. National Cancer Institute Web site. http://seer.cancer.gov/statfacts/html/mulmy.html.
Accessed October 21, 2012.
4. 4
Several Reasons for Limited Access to HCT Among
Elderly Patients With MM Have Been Proposed
• Possible reasons for discrepancy
– Patients ≥65 years historically not candidates for HCT1
– Elderly patients excluded from clinical trials2
– Comorbidity3
– Patient preference3
“Advanced age alone should not preclude the use of
effective cancer treatment that could improve quality of
life or extend meaningful survival.”4
‒NCCN Guidelines for Senior Adult Oncology
1. Palumbo A, Gay F. Hematology Am Soc Hematol Educ Program. 2009:566-577.
2. Kumar SK, et al. Am J Hematol. 2008;83(8):614-617.
3. Majhail NS, et al. Biol Blood Marrow Transplant. 2010;16(8):1070-1075.
4. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Senior Adult Oncology. v2.2012.
6. Original Article
Access to Hematopoietic Stem Cell
Transplantation
Effect of Race and Sex
Thomas V. Joshua, MS1; J. Douglas Rizzo, MD, MS2; Mei-Jie Zhang, PhD3; Parameswaran N. Hari, MD, MS2;
Seira Kurian, MD, MS, MPH4; Marcelo Pasquini, MD, MS2; Navneet S. Majhail, MD, MS5;
Stephanie J. Lee, MD, MPH6; and Mary M. Horowitz, MD, MS2
BACKGROUND: The purpose of the current study was to determine whether the use of hematopoietic stem cell
transplantation (HCT) to treat leukemia, lymphoma, or multiple myeloma (MM) differs by race and sex. METHODS:
The annual incidence of leukemia, lymphoma, and MM was estimated in the United States in people aged <70 years
by race and sex using the Surveillance, Epidemiology, and End Results (SEER) cancer registry between 1997 and
2002 and US census reports for the year 2000. The annual incidence of autologous, human leukocyte antigen (HLA)
identical sibling, and unrelated HCT performed in these groups was estimated using Center for International Blood
and Marrow Transplant Research data from 1997 through 2002. Logistic regression analysis was used to calculate the
age-adjusted odds ratio (OR) of receiving HCT for Caucasians versus African Americans and for men versus women.
RESULTS: The likelihood of undergoing HCT was found to be higher for Caucasians than for African Americans (OR,
1.40; 95% confidence interval [95% CI], 1.34-1.46). This difference existed for each type of HCT: autologous (OR, 1.24;
95% CI, 1.19-1.30), HLA identical sibling (OR, 1.59; 95% CI, 1.46-1.74), and unrelated donor (OR, 2.02; 95% CI, 1.75-2.33).
Overall, men were more likely than women to receive HCT (OR, 1.07; 95% CI, 1.05-1.1 [P < .0001]); however, this differ-
ence was found to be significant only for autologous HCT (OR, 1.10; 95% CI, 1.07-1.13 [P < .0001]). CONCLUSIONS:
HCT is more frequently used to treat leukemia, lymphoma, and MM in Caucasians than in African American individu-
als. African Americans have lower rates of both autologous and allogeneic HCT, indicating that donor availability can-
not fully explain the differences. Women are less likely than men to receive autologous HCT for reasons unexplained
by age or disease status. Cancer 2010;116:3469–76. V 2010 American Cancer Society.
C
KEYWORDS: access to care, hematopoietic stem cell transplantation, effect of race and sex, leukemia, lymphoma.
Hematopoietic stem cell transplantation (HCT) is a relatively new treatment modality. Its history began in the
late 1940s and early 1950s, when animal studies revealed the ability of donor bone marrow to restore hematopoiesis after
irradiation.1 The first successful HCTs in humans were performed in 1968.2-4 Procedure volume has increased rapidly
over the last few decades, with approximately 60,000 transplants performed worldwide in 2006.4 Although HCT has the
potential to increase survival for patients with many diseases, particularly hematologic malignancies, it is an intensive,
costly, and technically sophisticated procedure with a substantial risk of early morbidity and mortality.
Access to healthcare is defined as using affordable personal health services in a timely manner to achieve the best
health outcomes possible.5 The process of gaining access to care includes dynamic interactions between individuals with
diverse ethnic, cultural, and socioeconomic backgrounds; healthcare providers operating in a variety of practice patterns
with external constraints; and healthcare systems.6 HCT is an important treatment option for patients with leukemia,
lymphoma, and related disorders, offering the best chance for cure in several clinical situations.4,7,8 Limitations in access
to this procedure have substantial clinical, ethical, and policy implications.
Corresponding author: Thomas V. Joshua, MS, Center for Nursing Research, School of Nursing, Medical College of Georgia, 987 St. Sebastian Way, EC-4410,
Augusta, GA 30912; Fax: (706) 721-7049; tjoshua@mcg.edu
1
Center for Nursing Research, School of Nursing, Medical College of Georgia, Augusta, Georgia; 2Center for International Blood and Marrow Transplant Research,
Medical College of Wisconsin, Milwaukee, Wisconsin; 3Department of Biostatistics, Medical College of Wisconsin, Milwaukee, Wisconsin; 4Los Angeles County
Department of Public Health, Los Angeles, California; 5Department of Hematology/Oncology, University of Minnesota, Minneapolis, Minnesota; 6Department of
Hematology/Oncology, Fred Hutchinson Cancer Center, Seattle, Washington
DOI: 10.1002/cncr.25297, Received: November 10, 2009; Revised: January 20, 2010; Accepted: January 29, 2010, Published online May 24, 2010 in Wiley Inter-
Science (www.interscience.wiley.com)
Cancer July 15, 2010 3469
7. Original Article
Considerable variation exists in the distribution of Transplant Registry of the Medical College of Wisconsin
health and healthcare in the United States. In 2002, the and the National Marrow Donor Program (NMDP). The
Institute of Medicine published an authoritative report indi- CIBMTR is a voluntary consortium involving >500 trans-
cating that minorities are less likely than whites to receive plant centers in 54 countries. These transplant centers world-
needed routine and complex healthcare services across a wide contribute data regarding consecutive allogeneic and
broad array of diseases including cancer, cardiovascular dis- autologous HCTs to the CIBMTR. Participating centers are
ease, human immunodeficiency virus (HIV)/acquired im- required to report all transplants consecutively and compli-
munodeficiency syndrome (AIDS), diabetes, and mental ance is monitored through on-site audits. Computerized
illness.9 Since that report, the Agency for Healthcare checks for errors, physician review of submitted data, and
Research and Quality has published an annual National on-site audits of participating centers ensure the quality of
Healthcare Disparities Report (NHDR) to provide an over- the data. Patients are followed longitudinally, with yearly fol-
view of disparities in healthcare among racial, ethnic, and low-up. The NMDP facilitates approximately 95% of all
socioeconomic groups in the United States, and to track unrelated donor HCTs in the United States.
progress in reducing disparities.10 The 2006 NHDR sug- The SEER program of the National Cancer Insti-
27,28
gested that disparities remain prevalent between men and tute is an authoritative source of information regard-
women and among racial groups, including disparities in ing cancer incidence and survival in the United States.
cancer care.11 Several studies have indicated that men The SEER program collects and publishes cancer inci-
receive more early cancer detection tests than women in the dence and survival data from 14 population-based cancer
same practices,5,12,13 and cancer treatment outcomes are registries and 3 supplemental registries covering approxi-
poorer in African Americans.9-14 Outcome disparities may mately 26% of the US population.
be correlated with more advanced stage of disease at the
time of diagnosis, a phenomenon believed to be primarily Study Population
because of the underutilization of cancer screening. Some The population considered for this study included US
studies have suggested that lower socioeconomic status patients aged <70 years with acute lymphoblastic leuke-
resulting in reduced access to healthcare may be a major ex- mia (ALL), acute myelogenous leukemia (AML), chronic
planation for racial differences in cancer mortality.15-25 myelogenous leukemia (CML), non-Hodgkin lymphoma
The purpose of the current study was to determine (NHL), and MM who were treated between 1997 and
whether the use of HCT to treat leukemia, lymphoma, or 2002; these are the most common disease indications for
multiple myeloma (MM) differs by race and sex. We HCT. Patients aged >70 years were not considered
hypothesized that women and African Americans with these because few transplants are performed in older patients.
diseases are less likely to receive HCT. Although there may
be regional differences in healthcare availability,26 this study Statistical Analysis
examined utilization rates for the country as a whole. We calculated the annual number of incident cases of
ALL, AML, CML, NHL, and MM per 100,000 persons
MATERIALS AND METHODS based on the SEER population sampling frame between
The Center for International Blood and Marrow Trans- 1997 and 2002. First, incidence estimates were calculated
plant Research (CIBMTR) database was used to estimate from the SEER database separately for age group (ages
the annual number of HCTs performed in the United birth-19 years, 20-29 years, 30-39 years, 40-49 years,
States between 1997 and 2002. Data from the Surveil- 50-59 years, and 60-69 years), race (African American
lance, Epidemiology, and End Results (SEER)27,28 data- and Caucasian), and sex. This incidence rate was then
base and the US Census Bureau29 were used to estimate applied to US Census Bureau (year 2000) estimates for
the annual total number of new cases of each disease in numbers of persons in similar age, sex, and racial groups
the US population in the same time period. By using these to derive an estimated annual number of patients with
data, we estimated the rates (number of transplantations/ each disease in the US. The estimated annual numbers of
number of patients with disease) of HCT performed for autologous, human leukocyte antigen (HLA) identical
leukemia, lymphoma, and MM between 1997 and 2002. sibling, and unrelated donor HCTs performed during the
The CIBMTR is a research program formed in July same time period, and for each sex, racial, and age group,
2004 through an affiliation of the International Bone Mar- were calculated by retrieving the number of transplants
row Transplant Registry and Autologous Blood and Marrow registered with the CIBMTR between 1997 and 2002.
3470 Cancer July 15, 2010
8. Access to HCT: Effect of Race and Sex/Joshua et al
During this period, the CIBMTR collected an estimated Table 1. Characteristics of HCT Patients
55% of autologous, 50% of HLA identical sibling, and Variables Caucasian African Total
>90% of unrelated donor HCTs performed in the US No. (%) American No. (%)
(estimation is described in more detail elsewhere).30,31 Evaluable (%) Evaluable
Consequently, we applied an adjustment factor of No. of patients 25,068 (90) 2657 (10) 27,725
1.8 and 2.0, respectively, to the reported numbers of auto-
Sex
logous and HLA identical sibling HCTs. Male 14,807 (59) 1443 (54) 16,250 (59)
We then evaluated the rates of all HCTs as well as Female 10,261 (41) 1214 (46) 11,475 (41)
autologous, HLA identical sibling, and unrelated donor Year of transplant
HCTs by race and sex, for all diagnoses, and for each dis- 1997 3319 (13) 289 (11) 3608 (13)
1998 3916 (16) 403 (15) 4319 (16)
ease separately using logistic regression analysis adjusting 4236 (17) 468 (18) 4704 (17)
1999
for age. The rates of HCTs were calculated by dividing 2000 4427 (18) 463 (17) 4890 (18)
the number of estimated procedures by the number of 2001 4466 (18) 510 (19) 4976 (18)
2002 4704 (19) 524 (20) 5228 (19)
patients diagnosed with disease in the same age range.
When multiple comparisons were made, the P value of Age group at transplant, y
significance was considered to be .001 using Bonferroni Birth-19 2282 (9) 370 (14) 2652 (10)
20-29 1956 (8) 206 (8) 2162 (8)
adjustment. 30-39 3261 (13) 406 (15) 3667 (13)
In these analyses, we assumed that the sample of 40-49 5915 (24) 652 (25) 6567 (24)
50-59 7491 (30) 684 (26) 8175 (29)
patients reported to the CIBMTR was representative of
60-69 4163 (17) 339 (13) 4502 (16)
the total US population of HCT recipients. A sensitivity
Donor type
analysis was performed to assess the potential effect of
Auto HCT 13,758 (55) 1605 (60) 15,363 (55)
selective under-reporting of HCT for African Americans HLA sibling HCT 5230 (21) 501 (19) 5731 (21)
on the results of this study. In the initial analysis, we Unrelated HCT 6080 (24) 551 (21) 6631 (24)
assumed that 55% of all autologous HCTs and 50% of all Disease
allogeneic HCTs performed in the United States were AML 5247 (21) 458 (17) 5705 (21)
ALL 2340 (9) 245 (9) 2585 (9)
reported to CIBMTR, regardless of patient race. Data were
CML 2824 (11) 341 (13) 3165 (11)
reanalyzed after increasing the number of autologous and NHL 8936 (36) 546 (21) 9482 (34)
HLA identical sibling transplants for African Americans MM 5721 (23) 1067 (40) 6788 (24)
reported to the CIBMTR by 5%, 10%, 15%, and 20%. Graft type
Bone marrow 7544 (30) 635 (24) 8179 (30)
Peripheral blood 16,985 (68) 1895 (71) 18,880 (68)
Cord blood 539 (2) 127 (5) 666 (2)
RESULTS
A total of 27,725 patients registered with the CIBMTR HCT indicates hematopoietic stem cell transplantation; Auto HCT, autolo-
gous HCT; HLA sibling HCT, human leukocyte antigen identical sibling HCT;
met our selection criteria. Of these, 15,363 (55%) under- AML, acute myelogenous leukemia; ALL, acute lymphoblastic leukemia;
went autologous HCT, 5731 (21%) underwent HLA CML, chronic myelogenous leukemia; NHL, non-Hodgkin lymphoma; MM:
multiple myeloma.
identical sibling HCT, and 6631 (24%) underwent unre-
lated donor HCT. There were 25,068 (90%) patients
classified as Caucasian and 2657 (10%) classified as Afri-
can American. Approximately 59% were males. Pediatric Effect of Race
patients represented only 10% of patients who underwent Overall effect of race
transplantation and among those, 81% of the transplants Compared with African Americans, the age-adjusted
were for acute leukemia (AML and ALL). General charac- odds ratio (OR) of undergoing any type of HCT for all
teristics of the HCT population are presented in Table 1. diseases considered was higher for Caucasians (OR, 1.40;
By using these data and the adjustment factors described 95% confidence interval [95% CI], 1.35-1.46 [P
earlier, we estimated that there were approximately .0001]). A significantly higher OR of receiving HCT was
45,750 HCTs performed for the eligible diseases during noted for each type of HCT: autologous (OR, 1.24; 95%
the study period. During the same period of time, there CI, 1.19-1.30 [P .0001]), HLA identical sibling (OR,
were an estimated 273,853 patients diagnosed in the US 1.59; 95% CI, 1.46-1.74 [P .0001]), and unrelated do-
with the diseases considered in this analysis. nor (OR, 2.02; 95% CI, 1.75-2.33 [P .0001]) (Table 2).
Cancer July 15, 2010 3471
9. Original Article
Table 2. Age-Adjusted OR of Receiving HCT by Race and Sex
HCT Types and HCT Types and
ORs Caucasians ORs Males Versus
Versus African Females
Americans
Estimated Estimated Transplant OR (95% CI) P OR (95% CI) P
Annual US Annual HCTs Types
Incidence in the US
All diseases 45,643 7623 Overall HCT 1.40 (1.35-1.46) .0001 1.07 (1.05-1.1) .0001
4608 Autologous HCT 1.24 (1.19-1.30) .0001 1.10 (1.06-1.13) .0001
1910 HLA identical sibling HCT 1.59 (1.46-1.74) .0001 1.05 (0.99-1.10) .063
1105 Unrelated donor HCT 2.02 (1.75-2.33) .0001 0.94 (0.88-1.01) .11
ALL 3508 580 Overall HCT 1.01 (0.81-1.25) .97 1.08 (0.96-1.21) .21
40 Autologous HCT 0.74 (0.42-1.28) .28 0.7 (0.49-0.98) .04
262 HLA identical sibling HCT 0.93 (0.69-1.24) .61 1.17 (0.99-1.38) .06
278 Unrelated donor HCT 1.23 (0.87-1.73) .24 1.08 (0.90-1.28) .42
AML 5032 1459 Overall HCT 1.52 (1.35-1.71) .0001 0.83 (0.78-0.88) .0001
363 Autologous HCT 1.08 (0.90-1.3) .40 0.77 (0.69-0.85) .0001
694 HLA identical sibling HCT 1.44 (1.23-1.69) .0001 0.91 (0.83-0.99) .021
402 Unrelated donor HCT 2.29 (1.74-3.02) .0001 0.87 (0.77-0.98) .017
CML 2231 744 Overall HCT 1.42 (1.23-1.64) .0001 0.90 (0.82-0.98) .018
22 Autologous HCT 2.36 (0.99-5.64) .05 1.17 (0.77-1.78) .46
413 HLA identical sibling HCT 1.25 (1.05-1.49) .01 0.89 (0.80-0.99) .041
309 Unrelated donor HCT 1.45 (1.16-1.81) .001 0.92 (0.81-1.05) .21
NHL 27,960 2804 Overall HCT 2.12 (1.95-2.29) .0001 1.22 (1.17-1.26) .0001
2273 Autologous HCT 2.03 (1.86-2.22) .0001 1.18 (1.13-1.23) .0001
428 HLA identical sibling HCT 2.23 (1.89-2.79) .0001 1.45 (1.31-1.60) .0001
103 Unrelated donor HCT 3.14 (1.79-5.53) .0001 1.03 (0.84-1.27) .77
MM 6912 2036 Overall HCT 1.75 (1.64-1.86) .0001 1.1 (1.05-1.15) .0001
1910 Autologous HCT 1.72 (1.62-1.83) .0001 1.1 (1.05-1.15) .0001
113 HLA identical sibling HCT 1.55 (1.21-1.98) .0006 1.03 (0.86-1.23) .77
13 Unrelated donor HCT 3.24 (1.24-8.50) .016 1.64 (0.94-2.86) .08
OR indicates odds ratio; HCT, hematopoietic stem cell transplant; 95% CI, 95% confidence interval; HLA, human leukocyte antigen; ALL, acute lymphoblastic
leukemia; AML, acute myelogenous leukemia; CML, chronic myelogenous leukemia; NHL, non-Hodgkin lymphoma; MM, multiple myeloma.
Sensitivity analyses suggested that the results of this study 2.23; 95% CI, 1.89-2.79 [P .0001]), and unrelated do-
were robust, even in the conditional setting of 20% nor HCT (OR, 3.14; 95% CI, 1.79-5.53 [P .0001]).
under-reporting of HCTs in African Americans (OR, The OR of undergoing HCT for CML was higher for
1.15; 95% CI, 1.10-1.20). There were some differences Caucasians than for African Americans (OR, 1.42; 95%
observed by disease. CI, 1.23-1.64 [P .0001]). This difference was noted for
HLA identical sibling HCT (OR, 1.25; 95% CI, 1.05-
Effect of race by disease and type of HCT 1.49 [P ¼ .01]) and unrelated donor HCT (OR, 1.45;
The OR of undergoing HCT for MM was higher 95% CI, 1.16-1.81 [P ¼ .001]). Few patients (n ¼ 22)
for Caucasians than for African Americans (OR, 1.75; received autologous HCT. The OR of undergoing HCT
95% CI, 1.64-1.86 [P .0001]) (Table 2). This differ- for AML was higher for Caucasians than for African
ence was observed for autologous HCT (OR, 1.72; 95% Americans (OR, 1.52; 95% CI, 1.35-1.71 [P .0001]).
CI, 1.62-1.83 [P .0001]), HLA identical sibling HCT This difference was noted for HLA identical sibling HCT
(OR, 1.55; 95% CI, 1.21-1.98 [P ¼ .0006]), and unre- (OR, 1.44; 95% CI, 1.23-1.69 [P .0001]) and unre-
lated donor HCT (OR, 3.24; 95% CI, 1.24-8.50 lated donor HCT (OR, 2.29; 95% CI, 1.74-3.02 [P
[P ¼ .016]). The OR of undergoing HCT for NHL was .0001]), but not for autologous HCT (OR, 1.08; 95%
higher for Caucasians than for African Americans (OR, CI, 0.90-1.3). There was no difference noted with regard
2.12; 95% CI, 1.95-2.29 [P .0001]). This difference to the OR of undergoing HCT for ALL between Cauca-
was noted for autologous HCT (OR, 2.03; 95% CI, 1.86- sians and African Americans (OR, 1.01; 95% CI, 0.81-
2.22 [P .0001]), HLA identical sibling HCT (OR, 1.25 [P ¼ .97]).
3472 Cancer July 15, 2010
10. Access to HCT: Effect of Race and Sex/Joshua et al
Effect of Sex DISCUSSION
Overall effect of sex Decision-making regarding the performance of HCT
Overall, men were more likely than women to involves a complex interplay of factors. In general, catego-
receive HCT (OR, 1.07; 95% CI, 1.05-1.1 [P .0001]). ries of factors that may explain disparities in applied ther-
This difference was significant for autologous HCT (OR, apy include biologic factors (intrinsic variability in disease
1.10; 95% CI, 1.06-1.13 [P .0001]) but not for HLA natural history or response to therapy), patient factors
identical sibling (OR, 1.05; 95% CI, 0.99-1.10 [P ¼ .06]) (presence of comorbidities that prevent application of
or unrelated donor HCT (OR, 0.94; 95% CI, 0.88-1.01 therapy and patient preferences), healthcare systems fac-
[P ¼ .11]), and there were significant differences by dis- tors (health insurance and availability of healthcare facili-
ease. In particular, men were more likely than women to ties), and care process or discrimination factors (provider
undergo autologous HCT for MM or NHL. attitudes such as bias against minorities, greater clinical
uncertainty when understanding minorities’ symptoms
Effect of sex by disease and type of HCT and severity, or preconceived beliefs regarding minority
The OR of undergoing HCT for AML was lower behavior or health). Ideally, clinical needs and appropri-
for males than females; this difference was significant in ateness, biologic factors, and patient preferences should
all transplant types (Table 2). The OR of undergoing be the only considerations driving the therapeutic deci-
HCT for CML was lower for males than females; this dif- sion-making process. We assume that patient-related
ference was significant for HLA identical sibling HCT (other than preferences) and disease-related clinical factors
but not for autologous or unrelated donor HCT. The OR do not vary by race and sex such that indications for HCT
of undergoing HCT for NHL was higher for males than are not dramatically different in different racial and sex
for females; this difference was significant for autologous groups. We believe this is a reasonable assumption based
and HLA identical sibling HCT but not for unrelated do- on what is known about the diseases included in these
nor HCT. The OR of undergoing HCT for MM was analyses. The findings of the current study suggest a dis-
higher for males than females; this difference was signifi- parity in the rates of autologous and allogeneic HCT for
cant for autologous but not for HLA identical sibling or African Americans and females that should cause concern,
unrelated donor HCT. There was no difference noted in with the greatest disparity observed based on race. The
the OR of undergoing HCT for ALL between males and rates of HCT were higher in Caucasians than in African
females. Americans in nearly all subgroups examined, with ORs
2 in some categories.
Disparity in care could represent either underutiliza-
Affect of Adult Versus Pediatric Age Group tion in African Americans or overutilization in Cauca-
There were 2652 patients aged 20 years who were regis- sians. It could also be attributed to biologic differences.
tered with the CIBMTR and met our selection criteria in For example, the greater distribution of HLA types in
the study period. The majority of these children had AML African Americans and the smaller number of African
or ALL. We estimated that there were approximately Americans in volunteer donor registries make it more dif-
2955 HCTs performed for the eligible diseases during the ficult to find suitably matched donors for African Ameri-
study period. During the same period of time, there were cans in need of unrelated donor HCT. This may
an estimated 18,595 patients aged 20 years diagnosed in contribute to the lower rate of unrelated donor HCTs
the United States with the diseases considered in this anal- noted in this group. However, MM is a common indica-
ysis. There were no significant differences by race and sex tion for HCT. The preferred type of HCT for this disease
to report (data not shown) for this age group. is autologous, and during the 5-year time period spanned
by the current study, it became the most common indica-
Interaction of Sex and Race tion for autologous HCT.31 MM is twice as common in
We tested for interactions between sex and race by com- African Americans compared with Caucasians, but the
paring the overall and disease-specific OR of undergoing ORs of undergoing HCT for MM were found to be 72%
HCT in males versus females adjusting for race, and by higher for Caucasians. These lower rates of autologous
comparing the odds of HCT in Caucasians versus African HCT suggest that the disparity is best explained by under-
Americans, adjusting for sex. No significant interactions utilization of HCT in African Americans and cannot be
were evident. wholly attributed to donor availability.
Cancer July 15, 2010 3473
11. Original Article
The disparity in the use of HCT in men compared subject to very similar biases, given the similarities in
with women is less consistent than the disparity in use by reporting methods between the 2 databases. If individuals
race, with ORs closer to 1 and an increased OR noted in from a particular race were systematically misclassified in
men for some diseases and in women for others. A unify- any of these databases, it may misrepresent the true access
ing hypothesis for these differences is difficult to devise. rate for that particular race.
There were no significant differences in access to We assumed that family size, and therefore the num-
HCT for children noted based on sex or race. The lack of ber of potential sibling donors, was equal between Afri-
differential access to HCT for children compared with can-American and Caucasian populations. Because the
adults may be attributed, in part, to better governmental CIBMTR only collects data regarding HCT recipients,
(including state gap programs) and private insurance for we were unable to explore whether differences exist
children compared with adults. In addition, a larger per- between sex and racial groups with regard to rates of refer-
centage of children, particularly those with acute leuke- ral for consideration of HCT. Biologic-based racial differ-
mia, are referred early in their treatment course to larger ences in clinical presentation or response to initial therapy
pediatric medical centers and are treated on cooperative for disease may represent a partial explanation for the dis-
group trials, which may be more likely to afford them parity in HCT rates. Unfortunately, we did not have suffi-
access to HCT. cient data regarding disease status at the time of diagnosis
or comorbidities to determine whether this may have
Limitations affected consideration of HCT as a treatment option.
Several limitations of the current study should be consid- Although for the purposes of these analyses we have
ered. This analysis takes a national perspective in consid- assumed that the clinical appropriateness of HCT is simi-
ering racial disparities in HCT. The CIBMTR collected lar across the groups studied as described above, other
data on approximately 55% of all autologous transplants studies have suggested that African Americans are
and 50% of related donor transplants performed annually more likely to be diagnosed with an advanced stage of dis-
in the United States during the time period included in ease than whites, which would make them more likely to
the current study. Although regional differences may be of be candidates for aggressive therapy.32-34 However, if
greater interest because referral for HCT generally occurs true, such differences in stage at diagnosis should serve to
on a local/regional basis, the nature of the SEER and increase, not decrease, the ORs of HCT being performed
CIBMTR databases preclude subanalyses to present re- among African Americans compared with Caucasians.
gional differences in HCT. It is also possible that centers To the best of our knowledge, no data are currently
that perform more related donor or autologous HCTs in available regarding patient preferences for treatment, rates
African American individuals are under-represented in of refusal of HCT, or other sociocultural factors that
the CIBMTR. We addressed this incomplete denomina- could explain the differences in HCT observed in the cur-
tor of transplant activity in the United States by perform- rent study. Finally, there were insufficient data regarding
ing sensitivity analysis, the results of which suggested that healthcare process factors such as referring provider and
our conclusions were robust up to a moderate (20%) level transplant physician characteristics and practice patterns,
of under-reporting for specific racial groups. Because the geographic referral patterns, transplant center characteris-
CIBMTR captures data regarding nearly all unrelated do- tics, or socioeconomic characteristics of the patient to be
nor transplants in the United States, potential biases in incorporated into these analyses.
reporting are not an issue for that type of HCT and, in
fact, disparities in utilization were found to be highest for Conclusions
unrelated donor HCT. We observed a difference in the utilization of HCT for
An additional consideration is that attribution of leukemia, lymphoma, and MM by race, with Caucasians
patient race in the CIBMTR observational database is more likely to receive HCT than African Americans.
provided by the transplant centers. Centers may not use Importantly, lower HCT rates for African Americans
homogenous processes to identify and report the race of were noted for autologous HCT, indicating that donor
HCT recipients; these designations may not match self- availability cannot fully explain the differences observed.
reported race and may contribute to reporting bias. How- Differences by sex were less striking. We believe these dif-
ever, it appears likely that reporting of race within the ferences represent substantial underutilization of HCT in
SEER database during the same time period would be African Americans. The identification of disparities
3474 Cancer July 15, 2010
12. Access to HCT: Effect of Race and Sex/Joshua et al
should serve as the motivation to further understand their REFERENCES
cause, and their elimination whenever they are inappro- 1. Serna DS, Lee SJ, Zhang MJ, et al. Trends in survival rates
priate. Further study is essential to better characterize and after allogeneic hematopoietic stem-cell transplantation for
explain disparities in access to HCT. Research should acute and chronic leukemia by ethnicity in the United States
and Canada. J Clin Oncol. 2003;21:3754-3760.
explore whether patient or provider preferences, sociocul- 2. Bach FH, Albertini RJ, Joo P, Anderson JL, Bortin MM.
tural or socioeconomic factors, or healthcare process fac- Bone-marrow transplantation in a patient with the Wiskott-
tors explain disparities in access to HCT, and whether Aldrich syndrome. Lancet. 1968;2:1364-1366.
these factors are modifiable. While waiting for further 3. Gatti RA, Meuwissen HJ, Allen HD, Hong R, Good RA.
Immunological reconstitution of sex-linked lymphopenic
research to better understand disparate access to HCT, immunological deficiency. Lancet. 1968;2:1366-1369.
the medical community should work at all levels to elimi- 4. Center for International Blood and Marrow Transplant
nate these disparities. Research. CIBMTR Progress Report: January-December
2007. Milwaukee, WI: Center for International Blood and
Marrow Transplant Research; 2007:5.
CONFLICT OF INTEREST DISCLOSURES 5. Mandelblatt JS, Yabroff KR, Kerner JF. Equitable access to
cancer services: a review of barriers to quality care. Cancer.
The Center for International Blood and Marrow Transplant 1999;86:2378-2390.
Research (CIBMTR) is supported by Public Health Service 6. Mitchell JM, Meehan KR, Kong J, Schulman KA. Access to
Grant/Cooperative Agreement U24-CA76518 from the bone marrow transplantation for leukemia and lymphoma:
National Cancer Institute (NCI); the National Heart, Lung the role of sociodemographic factors. J Clin Oncol.
and Blood Institute (NHLBI); and the National Institute of 1997;15:2644-2651.
Allergy and Infectious Diseases (NIAID); a Grant/Cooperative
7. Copelan EA. Hematopoietic stem-cell transplantation. N
Agreement 5U01HL069294 from NHLBI and NCI; contract
Engl J Med. 2006;354:1813-1826.
HHSH234200637015C with the Health Resources and Services
8. Lennard AL, Jackson GH. Stem cell transplantation. BMJ.
Administration (HRSA/DHHS); and 2 grants (N00014-06-1-
2000;321:433-437.
0704 and N00014-08-1-0058) from the Office of Naval
Research, as well as grants from AABB; Aetna; American Society 9. Smedley BD, Stith AY, Nelson AR. Unequal Treatment:
for Blood and Marrow Transplantation; Amgen, Inc; an anony- Confronting Racial and Ethnic Disparities in Health Care.
mous donation to the Medical College of Wisconsin; Astellas Washington, DC: National Academies Press; 2003.
Pharma US, Inc; Baxter International, Inc; Bayer HealthCare 10. Agency for Healthcare Research and Quality. National
Pharmaceuticals; Be the Match Foundation; Biogen IDEC; Bio- Healthcare Disparities Report. Rockville, MD: Agency for
Marin Pharmaceutical, Inc; Biovitrum AB; BloodCenter of Wis- Healthcare Research and Quality; 2006.
consin; Blue Cross and Blue Shield Association; Bone Marrow 11. Long JA, Chang VW, Ibrahim SA, Asch DA. Update on
Foundation; Canadian Blood and Marrow Transplant Group; the health disparities literature. Ann Intern Med. 2004;141:
CaridianBCT; Celgene Corporation; CellGenix, GmbH; Centers 805-812.
for Disease Control and Prevention; Children’s Leukemia 12. Shavers VL, Harlan LC, Stevens JL. Racial/ethnic variation
Research Association; ClinImmune Labs; CTI Clinical Trial and in clinical presentation, treatment, and survival among
Consulting Services; Cubist Pharmaceuticals; Cylex Inc; Cyto- breast cancer patients under age 35. Cancer. 2003;97:134-
Therm; DOR BioPharma, Inc; Dynal Biotech, an Invitrogen 147.
Company; Eisai, Inc; Enzon Pharmaceuticals, Inc; European 13. Demark-Wahnefried W, Strigo T, Catoe K, et al. Knowl-
Group for Blood and Marrow Transplantation; Gamida Cell, edge, beliefs, and prior screening behavior among blacks
Ltd; GE Healthcare; Genentech, Inc; Genzyme Corporation; and whites reporting for prostate cancer screening. Urology.
Histogenetics, Inc; HKS Medical Information Systems; Hospira, 1995;46:346-351.
Inc; Infectious Diseases Society of America; Kiadis Pharma; 14. Robinson KD, Kimmel EA, Yasko JM. Reaching out to the
Kirin Brewery Co., Ltd; The Leukemia and Lymphoma Society; African American community through innovative strategies.
Merck Company; The Medical College of Wisconsin; MGI Oncol Nurs Forum. 1995;22:1383-1391.
Pharma, Inc; Michigan Community Blood Centers; Millennium 15. Vernon SW, Heckel V, Jackson GL. Medical outcomes of
Pharmaceuticals, Inc; Miller Pharmacal Group; Milliman USA, care for breast cancer among health maintenance organiza-
Inc; Miltenyi Biotec, Inc; National Marrow Donor Program; tion and fee-for-service patients. Clin Cancer Res. 1995;1:
Nature Publishing Group; New York Blood Center; Novartis 179-184.
Oncology; Oncology Nursing Society; Osiris Therapeutics, Inc; 16. Zaloznik AJ. Breast cancer stage at diagnosis: Caucasians
Otsuka America Pharmaceutical, Inc; Pall Life Sciences; Pfizer versus Afro-Americans. Breast Cancer Res Treat. 1995;34:
Inc; Saladax Biomedical, Inc; Schering Corporation; Society for 195-198.
Healthcare Epidemiology of America; StemCyte, Inc; StemSoft 17. Mehta P, Pollock BH, Nugent M, Horowitz M, Wingard
Software, Inc; Sysmex America, Inc; Teva Pharmaceutical Indus- JR. Access to stem cell transplantation: do women fare as
tries; THERAKOS, Inc; Thermogenesis Corporation; Vidacare well as men? Am J Hematol. 2003;72:99-102.
Corporation; Vion Pharmaceuticals, Inc; ViraCor Laboratories; 18. Liu JR, Conaway M, Rodriguez GC, Soper JT, Clarke-Pear-
ViroPharma, Inc; and Wellpoint, Inc. The views expressed in son DL, Berchuck A. Relationship between race and interval
this article do not reflect the official policy or position of the to treatment in endometrial cancer. Obstet Gynecol. 1995;
National Institute of Health, the Department of the Navy, the 86(4 pt 1):486-490.
Department of Defense, or any other agency of the US 19. Schapira MM, McAuliffe TL, Nattinger AB. Treatment of
Government. localized prostate cancer in African-American compared
Cancer July 15, 2010 3475
13. Original Article
with Caucasian men. Less use of aggressive therapy for com- Public-Use, Nov 2004 Sub (1973-2002). Bethesda, MD:
parable disease. Med Care. 1995;33:1079-1088. National Cancer Institute, Division of Cancer Control
20. King TE Jr, Brunetta P. Racial disparity in rates of surgery and Population Sciences, Surveillance Research Program,
for lung cancer. N Engl J Med. 1999;341:1231-1233. Cancer Statistics Branch; released April 2005, based on
21. Bach PB, Schrag D, Brawley OW, Galaznik A, Yakren S, the November 2004 submission. Available at: www.seer.
Begg CB. Survival of blacks and whites after a cancer diag- cancer.gov.
nosis. JAMA. 2002;287:2106-2113. 29. US Census Bureau. Race and Gender Data. Available at:
22. Demark-Wahnefried W, Schildkraut JM, Iselin CE, et al. http://www.census.gov 2000. Accessed June 11, 2005.
Treatment options, selection, and satisfaction among African 30. Nietfeld JJ, Pasquini MC, Logan BR, Verter F, Horowitz
American and white men with prostate carcinoma in North MM. Lifetime probabilities of hematopoietic stem cell trans-
Carolina. Cancer. 1998;83:320-330. plantation in the U.S. Biol Blood Marrow Transplant.
23. Espey D, Paisano R, Cobb N. Regional patterns and trends 2008;14:316-322.
in cancer mortality among American Indians and Alaska 31. Pasquini M. Current use and outcome of hematopoietic
Natives, 1990-2001. Cancer. 2005;103:1045-1053. stem cell transplantation: part I – CIBMTR Summary
24. Du W, Simon MS. Racial disparities in treatment and sur- Slides, 2005. CIBMTR Newsletter [serial online]. 2005;12:
vival of women with stage I-III breast cancer at a large aca- 5-8.
demic medical center in metropolitan Detroit. Breast Cancer 32. U.S. Cancer Statistics Working Group. United States Can-
Res Treat. 2005;91:243-248. cer Statistics: 1999-2005. Incidence and Mortality Web-
25. Shavers VL, Brown ML. Racial and ethnic disparities in the based Report. Atlanta, GA: U.S. Department of Health and
receipt of cancer treatment. J Natl Cancer Inst. 2002;94: Human Services, Centers for Disease Control and Preven-
334-357. tion and National Cancer Institute; 2009. Available at:
26. Asch DA, Armstrong K. Aggregating and partitioning popu- www.cdc.gov/uscs. Accessed June 11, 2005.
lations in health care disparities research: differences in per- 33. North American Association of Central Cancer Registries,
spective. J Clin Oncol. 2007;25:2117-2121. Inc. Average-Annual Registry-Specific Cancer Incidence by
27. Surveillance, Epidemiology, and End Results (SEER) Pro- Race, Ethnicity, and Sex; 2009v2. Springfield, IL: North
gram. Cancer incidence and survival among children and American Association of Central Cancer Registries, Inc;
adolescents: United States SEER Program 1975-1995. In: Year. Available at: http://www.naaccr.org/filesystem/pdf/CI-
Ries LAG, Gurney JG, Linet M, Tamra T, Young JL, NA2009v2.world.pdf. Accessed January 17, 2009.
Bunin GR, eds. NIH Pub. No 99-4649. Bethesda, MD: 34. Parker SL, Johnston Davis K, Wingo PA, Ries LAG, Heath
National Cancer Institute; 1999. CW. Cancer statistics by race and ethnicity. CA Cancer J Clin.
28. Surveillance, Epidemiology, and End Results (SEER) Pro- 1998;48:31-48. Available at: http://caonline.amcancersoc.
gram. SEER*Stat (6.4) Database: Incidence-SEER 9 Regs org/cgi/reprint/48/1/31.pdf. Accessed January 17, 2009.
3476 Cancer July 15, 2010
14. Race and Outcomes of Autologous Hematopoietic Cell
Transplantation for Multiple Myeloma
Parameswaran N. Hari,1 Navneet S. Majhail,2,3 Mei-Jie Zhang,1 Anna Hassebroek,2
Fareeha Siddiqui,4 Karen Ballen,5 Asad Bashey,6 Jenny Bird,7 Cesar O. Freytes,8 John Gibson,9
Gregaory Hale,10 Leona Holmberg,11 Ram Kamble,12 Robert A. Kyle,13 Hillard M. Lazarus,14
Charles F. LeMaistre,15 Fausto Loberiza,16 Angelo Maiolino,17 Philip L. McCarthy,18
Gustavo Milone,19 Nancy Omondi,20 Donna E. Reece,21 Matthew Seftel,22 Michael Trigg,23
David Vesole,24 Brendan Weiss,25 Peter Wiernik,26 Stephanie J. Lee,1 J. Douglas Rizzo,1
Paulette Mehta27
Blacks are twice as likely to develop and die from multiple myeloma (MM), and are less likely to receive an
autologous hematopoietic-cell transplant (AHCT) for MM compared to Whites. The influence of race on
outcomes of AHCT for MM is not well described. We compared the probability of overall survival (OS), pro-
gression-free survival (PFS), disease progression, and nonrelapse mortality (NRM) among Black (N 5 303)
and White (N 5 1892) recipients of AHCT for MM, who were reported to the Center for International
Blood and Marrow Transplant Research (CIBMTR) from 1995 to 2005. The Black cohort was more likely
to be female, and had better Karnofsky performance scores, but lower hemoglobin and albumin levels at di-
agnosis. Black recipients were younger and more likely to be transplanted later in their disease course. Dis-
ease stage and treatment characteristics prior to AHCTwere similar between the 2 groups. Black and White
recipients had similar probabilities of 5-year OS (52% versus 47%, P 5.19) and PFS (19% versus 21%, P 5.64)
as well as cumulative incidences of disease progression (72% versus 72%, P 5.97) and NRM (9% versus 8%,
P 5.52). In multivariate analyses, race was not associated with any of these endpoints. Black recipients of
AHCT for MM have similar outcomes compared to Whites, suggesting that the reasons underlying lower
rates of AHCT in Blacks need to be studied further to ensure equal access to effective therapy.
Biol Blood Marrow Transplant 16: 395-402 (2010) Ó 2010 American Society for Blood and Marrow Transplantation
KEY WORDS: Autologous hematopoietic cell transplantation, Multiple myeloma, Race, Survival, Progres-
sion-free survival
From the 1Center for International Blood and Marrow Transplant Rio de Janeiro, Brazil; 18Roswell Park Cancer Institute, Buffalo
Research, Medical College of Wisconsin, Milwaukee, Wiscon- New York; 19Angelica Ocampo-Hospital and Research Center,
sin; 2Center for International Blood and Marrow Transplant Fundaleu Buenos Aires, Argentina; 20National Marrow Donor
Research, National Marrow Donor Program, Minneapolis, Program, Minneapolis, Minnesota; 21University of Toronto,
Minnesota; 3University of Minnesota, Minneapolis Minnesota; Toronto, Ontario, Canada; 22CancerCare Manitoba, Manitoba,
4
Medical College of Wisconsin, Milwaukee, Wisconsin; 5Mas- Canada; 23Merck Co. Inc., Wilmington, Delaware; 24Loyola
sachusetts General Hospital, Boston, Massachusetts; 6Blood University Health System, Maywood, Illinois; 25Walter Reed
and Marrow Transplant Group of Georgia, Atlanta, Georgia; Army Medical Center, Washington, DC; 26New York Medical
7
Bristol Haematology and Oncology Centre, Bristol, United College, Bronx, New York; and 27University of Arkansas, Little
Kingdom; 8South Texas Veterans Health Care System and Uni- Rock, Arkansas.
versity of Texas Health Center at San Antonio, San Antonio, Financial disclosure: See Acknowledgments on page 401.
Texas; 9Royal Prince Alfred Hospital, Camperdown, Australia; Correspondence and reprint requests: Parameswaran Hari, MD,
10
A Children’s Hospital, Saint Petersburg, Florida; 11Fred MS, CIBMTR, Medical College of Wisconsin, P.O. Box
Hutchinson Cancer Research Center, Seattle, Washington; 26509, 8701 Watertown Plank Road, Milwaukee, WI 53226
12
Baylor College of Medicine, Houston, Texas; 13Mayo Clinic, (e-mail: phari@mcw.edu).
Rochester Minnesota; 14University Hospitals Case Medical Received September 11, 2009; accepted November 8, 2009
Center, Cleveland, Ohio; 15Texas Transplant Institute, San An- Ó 2010 American Society for Blood and Marrow Transplantation
tonio, Texas; 16University of Nebraska Medical Center, Omaha, 1083-8791/10/163-0012$36.00/0
Nebraska; 17Hospital Univarstario Clementino Frago Filho, doi:10.1016/j.bbmt.2009.11.007
395
15. 396 P. N. Hari et al. Biol Blood Marrow Transplant 16:395-402, 2010
BACKGROUND Wisconsin in Milwaukee or the National Marrow
Donor Program (NMDP) Coordinating Center in
Multiple myeloma (MM) remains an incurable dis- Minneapolis. Subjects are followed longitudinally,
ease, although prognosis has improved in the past with yearly follow-up. Computerized checks for
decade [1,2]. It is the most common hematologic ma- errors, physicians’ review of submitted data, and on-
lignancy among Blacks, and is the only hematologic site audits of participating centers ensure data quality.
malignancy that is more frequent in this racial group Observational studies conducted by the CIBMTR are
compared with Whites. In the United States, MM done with a waiver of informed consent and in compli-
and its precursor disease monoclonal gammopathy of ance with HIPAA regulations as determined by the
undetermined significance (MGUS) are twice as com- Institutional Review Board and the Privacy Officer of
mon in Blacks (annual incidence of 14.4/100,000 in the Medical College of Wisconsin.
men and 9.8/100,000 in women compared with 6.6/
100,000 in White men and 4.1/100,000 in White
Patients
women) [1,3-7]. Proposed factors to explain the
increased incidence among Blacks include socioeco- The study included 2195 (303 Black and 1892
nomic factors, greater exposure to hazardous materials, White) adult (aged $18 years) recipients of AHCT
genetic predisposition, greater degree of background for MM who were transplanted between January 1995
antigenic stimulation, and a greater prevalence of obe- and June 2005 (Table 1). Only recipients of peripheral
sity [8-10]. Mortality rates from MM in the United blood (PB) AHCT were included in this study; patients
States are twice as high for Blacks compared to Whites who had received planned tandem AHCT (N 5 582)
(8.3/100,000 for men and 6.0/100,000 for women com- were excluded. Centers obtained information about
pared to 4.3/100,000 and 2.8/100,000 for White men patient race and then reported it to the CIBMTR.
and women, respectively) [11].
Socioeconomic factors that may have an impact on Statistical Methods
access to cancer therapy and therapeutic choices in- Patient-, disease-, and treatment-related factors
clude place of residence, distance from care centers, un- were compared between the Black and White cohorts,
employment, availability and quality of health using a chi-square test for categorical and a Kruskal-
insurance, poor nutrition, exposure to infectious Wallis test for continuous variables. Outcomes analyzed
agents, lower educational level, and annual income included nonrelapse mortality (NRM), relapse/pro-
[12,13]. Prior comparisons have drawn conflicting con- gression, progression-free survival (PFS), and overall
clusions on treatment outcomes among Blacks com- survival (OS). NRM was defined as death occurring in
pared with White patients with MM. Savage et al. the absence of relapse or progression of MM following
[13,14] found that Black patients had shorter survival AHCT. Relapse/progression was defined according to
times following similar therapy for MM. Presentation standard criteria [20]. Chemotherapy sensitivity was de-
at later stages of disease, socioeconomic factors, or dif- fined as achievement of a partial or complete response
ferential access to care were thought to explain this dis- (PR, CR) to pretransplant therapy. PFS was defined as
parity. Other investigators have suggested that these survival without disease progression or relapse. Patients
disparities in outcomes are primarily because of biolog- alive and with no evidence of disease progression or re-
ical characteristics [15,16]. lapse were censored at the time of last follow-up. The
Randomized clinical trials support the use of autol- survival interval variable was defined as time from the
ogous hematopoietic-cell transplant (AHCT) as a stan- date of transplant to the date of death or last contact
dard therapy for MM [17,18]. We have previously and summarized by a survival curve. Probabilities of
shown that Blacks are less likely to receive AHCT for OS and PFS were calculated using the Kaplan-Meier es-
MM compared with their age- and sex-matched White timator [21,22]. NRM and relapse/progression were
counterparts [19]. In the current study, we compared calculated using cumulative incidence estimates. The
outcomes between Black and White patients receiving log-rank test was used for univariate comparisons.
AHCT for MM to determine if disparate post trans- Multivariate Cox proportional hazards regression
plant outcomes validate lower AHCT use in Blacks. was used to examine the outcomes between Black
and White patient cohorts and to identify risk factors
PATIENTS AND METHODS associated with outcomes [23]. A stepwise forward
selection multivariate model was built to identify
The Center for International Blood and Marrow covariates that influenced outcomes. Any covariate
Transplant Research (CIBMTR) consists of a volun- with a value of P .05 was considered significant.
tary working group of more than 450 transplant The proportionality assumption for Cox regression
centers worldwide. Centers contribute detailed data was tested by adding a time-dependent covariate for
on consecutive allogeneic and autologous transplants each risk factor and each outcome. Tests indicated
to a statistical center at either the Medical College of that all variables met the proportional hazards
16. Biol Blood Marrow Transplant 16:395-402, 2010 Race and Outcomes of AHCT for MM 397
Table 1. Patient Characteristics
White Black
Variable N (%) N (%) P-value
Number of patients 1892 303
Age median (range), years 57 (27-80) 55 (27-74) .001
Age group at transplant, years .002
50 396 (21) 88 (29)
50-64 1111 (59) 172 (57)
$ 65 385 (20) 43 (14)
Male sex 1136 (60) 164 (54) .05
Karnofsky score pretransplant .005
$90 1153 (61) 210 (69)
Hypertension .001
Yes 471 (25) 143 (47)
Diabetes .001
Yes 169 (9) 50 (17)
Body Mass Index .01
Underweight/normal (25) 557 (29) 67 (22)
Overweight (25-29.9) 741 (39) 120 (40)
Obese/morbidly obese ($30) 594 (31) 116 (38)
Disease related
Durie-Salmon stage at diagnosis .25
I 203 (11) 25 (8)
II 562 (30) 101 (33)
III 1127 (60) 177 (58)
Immunochemical subtype of myeloma .34
IgG 1003 (53) 173 (57)
IgA 359 (19) 45 (15)
Light chain 329 (17) 54 (18)
Others/unknown 125 (11) 16 (10)
Albumin level at diagnosis .05
3.5 g/dL 732 (39) 101 (33)
Hemoglobin at diagnosis 10 g/dL .001
10 g/dL 552 (29) 135 (45)
Creatinine at diagnosis .09
1.5 mg/dL 361 (19) 74 (24)
B-2 microglobulin level at diagnosis .83
$5.5 mg/L 195 (10) 31 (10)
Prior chemotherapy regimens .78
MP ± others 334 (18) 50 (17)
VAD ± others (not MP) 1104 (58) 182 (60)
Cy ± others 300 (16) 52 (17)
Corticosteroids ± others 154 (8) 19 (6)
Number of lines of chemotherapy§ .29
1 1125 (59) 167 (55)
2 536 (28) 99 (33)
2 231 (12) 37 (12)
Sensitive to chemotherapy prior to transplant .83
Sensitive 1434 (76) 228 (75)
Disease status at time of transplant .67
Complete remission/partial remission 1396 (74) 231 (76)
Treatment related
Time from diagnosis to transplant median (range), months 8 (1-249) 9 (2-217) .001
Time from diagnosis to transplant .001
12 months 1364 (72) 190 (63)
$12 months 528 (28) 113 (37)
Conditioning regimen .7
Melphalan only 1417 (75) 223 (74)
Melphalan + TBI ± others 204 (11) 35 (12)
Bu-Cy ± others (not TBI, not melphalan) 271 (15) 45 (15)
Median follow-up of survivors, median (range) 61 (1-145) 51 (1-132)
MP indicates Melphalan + Prednisone; VAD, vincristine + dexamethasone + adriamycin; Cy, cyclophosphamide; Bu, busulfan; TBI, total body irradiation;
Eval, evaluable.
§ Excludes stem cell priming.
assumption. Results were expressed as relative risks The variables considered in multivariate analyses are
(RR). Any risk factors found to be significant were ad- summarized in Table 2. Analyses were performed us-
justed in the final Cox model. The main effect tested ing SAS software, version 9.1 (SAS Institute, Cary,
(ie, Black versus White) was included in all models. NC).
17. 398 P. N. Hari et al. Biol Blood Marrow Transplant 16:395-402, 2010
Table 2. Variables Tested in Multivariate Analysis
Main effect variable:
Race/ethnicity: White* versus Black
Patient-related variables:
Age: 50* versus 50-64 versus $ 65
Sex: Male* versus Female
Karnofsky performance status at transplant: 90% versus $90%* versus
missing
Body mass index: underweight/normal* versus overweight versus obese/
morbidly obese
Hypertension anytime prior to transplant: yes* versus no
Diabetes anytime prior to transplant: yes* versus no
History of smoking prior to transplant: yes* versus no
Creatinine 1.5 mg/dL versus #1.5* mg/dL at diagnosis
MM subtype: IgG versus IgA versus Light chain versus others/unknown
Figure 1. Cumulative incidence of nonrelapse mortality.
Disease-related variables:
Durie-Salmon stage at diagnosis: I* versus II versus III
Number of lines of chemotherapy: 1* versus 2 versus 2 NRM and Relapse/Progression
Sensitivity to chemotherapy prior to transplant: sensitive* versus others Figure 1 shows the cumulative incidence of NRM.
Disease status prior to transplant: complete remission/partial remission*
versus others (includes minimal response, no response, stable disease, The cumulative incidence of NRM was similar in both
relapse/progressive disease and unknown) groups. At 1 year, it was 5% (95% confidence interval
Prior chemotherapy regimens: MP* versus VAD versus Cy ± others versus [CI] 4%-6%) in Whites versus 3% (95% CI 2%-6%)
Corticosteroids ± others
in Blacks. At 5 years, it was 8% (95% CI 7%-9%) ver-
Transplant-related variables:
Time from diagnosis to transplant: 12 months* versus others
sus 9% (95% CI 6%-14%) in Whites and Blacks, re-
Conditioning regimen: melphalan only* versus melphalan + TBI ± others spectively. In multivariate analysis (Table 3), race
versus Bu-Cy ± others (not TBI, not melphalan) was not associated with NRM. Factors associated
Purging: yes* versus no
Year of transplant: 1995-2001 versus 2002-2005*
with an increased risk of NRM were age $65 years,
KPS 90, and AHCT prior to 2002.
MP indicates Melphalan + Prednisone; VAD, vincristine + dexametha- Figure 2 shows cumulative incidence of relapse/
sone + adriamycin; Cy, cyclophosphamide; Bu, busulfan; TBI, total
body irradiation. progression. The cumulative incidence of relapse/pro-
*Reference group. gression was similar in both groups. At 1 year, it was
27% (95% CI 25%-29%) in Whites versus 28% (95%
CI 23%-34%) in Blacks. At 5 years it was 72% (95%
RESULTS CI 69%-74%) versus 72% (95% CI 65%-78%) in
Whites and Blacks, respectively. In multivariate analysis
Patient Characteristics (Table 3), race was not associated with disease relapse or
progression. Factors associated with an increased risk of
Table 1 shows the characteristics of all patients
relapse included KPS score 90, Durie-Salmon stage
evaluated. Median ages at AHCT were 55 years for
III at diagnosis, receipt of 3 or more lines of chemother-
Black compared to 57 years for White patients
apy before AHCT, lack of chemosensitive disease prior
(P .001). The Black cohort had a higher proportion
to AHCT, AHCT $12 months from diagnosis, and
of females and patients with Karnofsky performance
later year of AHCT.
status scores (KPS) .90 (69% versus 61%, P 5 .005).
Blacks were more likely to have comorbidities such
as hypertension (47% versus 25%, P .001), diabetes PFS and OS
mellitus (l7% versus 9%, P .001), and obesity (38% Figure 3 shows the probability of PFS. The 1- and
versus 31%, P 5 .01). No statistically significant dif- 5-year probabilities of PFS were similar in both groups.
ferences in disease stage or MM subtype were identi- At 1 year, it was 68% (95% CI 66%-70%) in Whites
fied. Blacks were also more likely to have a lower versus 68% (95% CI 63%-74%) in Blacks. At 5 years,
hemoglobin (Hb 10 g/dL in 45% versus 29%, P it was 21% (95% CI 18%-23%) versus 19% (95% CI
.001) at diagnosis. No significant differences in the 14%-25%) in Whites and Blacks, respectively. In mul-
levels of serum creatinine, beta-2 microglobulin, cal- tivariate analysis (Table 4), race was not associated with
cium, or marrow plasmacytosis were identified. The PFS.
cohorts did not differ with respect to the type and Figure 4 shows the probability of OS after AHCT.
number of prior therapies or sensitivity to therapies The 1- and 5-year survival rates were also similar be-
applied before transplantation. Blacks were trans- tween the 2 cohorts. At 1 year, it was 87% (95% CI
planted later in the disease course, with 37% receiving 85%-88%) in Whites versus 90% (95% CI 87%-93%)
AHCT a year or more from diagnosis versus 28% in in Blacks. At 5 years, it was 47% (95% CI 44%-49%)
Whites (P .001). There were no significant differ- versus 52% (95% CI 45%-59%) in Whites and Blacks,
ences in conditioning regimens used or the receipt of respectively. In multivariate analysis (Table 4), race was
a salvage second AHCT. not a significant predictor of survival.
18. Biol Blood Marrow Transplant 16:395-402, 2010 Race and Outcomes of AHCT for MM 399
Table 3. Multivariate Analysis for Relapse and Nonrelapse Mortality
Relapse Nonrelapse mortality
Variable N RR P-Value N RR P-Value
Race
White 1850 1.00 1850 1.00
Black 296 0.92 (0.78-1.08) P 5.28 296 1.16 (0.75-1.80) P 5.51
Patient age, years
50 475 1.00 P .001
50-64 1253 1.55 (1.01-2.39) P 5.05
$65 418 3.50 (2.17-5.65) P .001
Karnofsky Score prior to conditioning
90 815 1.00 815 1.00
$90 1331 0.88 (0.79-0.98) P 5.02 1331 0.72 (0.53-0.98) P 5.03
Durie-Salmon stage at diagnosis
I 222 1.00 P .001 222 1.00 P 5.004
II 652 1.23 (1.00-1.51) P 5.05 652 0.61 (0.35-1.06) P 5.08
III 1272 1.54 (1.27-1.87) P .001 1272 1.16 (0.71-1.88) P 5.56
Number of lines of chemotherapy‡
1 1256 1.00 P 5.001
2 628 1.12 (0.99-1.27) P 5.07
2 262 1.39 (1.16-1.66) P .001
Sensitivity to chemotherapy prior
to transplant
Other 522 1.00
Sensitive 1624 0.76 (0.67-0.85) P .001
Time from diagnosis to transplant
12 months 1519 1.00
$12 months 627 1.19 (1.04-1.35) P 5.009
Year of transplant
1995-2001 1331 1.00 1331 1.00
2002-2005 815 1.17 (1.04-1.31) P 5.008 815 0.56 (0.39-0.81) P 5.002
RR indicates relative risk.
‡Excludes stem cell priming.
PFS and OS were worse in patients with older age These results concur with observations in other studies
at AHCT (.50 years), KPS score 90, higher Durie- of nontransplant therapy that the disparity in out-
Salmon stage, those who received 2 or more lines of comes for MM disappears when Blacks receive identi-
therapy prior to AHCT, AHCT $12 months from di- cal therapy [24].
agnosis, and chemotherapy resistant disease (Table 4). Several investigators have shown that Blacks have
OS was also lower in patients who underwent AHCT outcomes similar to Whites when given the same non-
prior to 2002. transplant treatment for MM. Rohatgi et al. [25]
The major cause of mortality in both cohorts was showed that Blacks were less likely to receive chemo-
relapse or progression of MM that accounted for therapy, but they responded with similar outcomes
72% of all deaths. when given similar nontransplant therapy for MM.
In the pretransplant era, Modiano et al. [26] retrospec-
DISCUSSION tively evaluated the impact of race in the results of the
SWOG 8829 study of conventional chemotherapy for
Our analysis establishes that Black and Whites MM. From 99 study sites in the United States, 116
have very similar outcomes after AHCT for MM. Black and 467 White patients were shown to have
Figure 2. Cumulative incidence of disease relapse and progression. Figure 3. Probability of progression-free survival.
19. 400 P. N. Hari et al. Biol Blood Marrow Transplant 16:395-402, 2010
Table 4. Multivariate Analysis for Overall Survival and Progression-Free Survival
Overall Survival Progression-Free Survival
Variable N RR P-Value N RR P-Value
Race
White 1892 1.00 1850 1.00
Black 303 0.94 (0.78-1.13) P 5.50 296 0.94 (0.81-1.09) P 5.39
Patient age, years
50 484 1.00 P .0001 475 1.00 P 5.03
50-64 1283 1.26 (1.09-1.46) P 5.002 1253 1.12 (0.99-1.27) P 5.08
$65 428 1.52 (1.26-1.83) P .0001 418 1.24 (1.06-1.46) P 5.007
Karnofsky Score prior to conditioning
90 832 1.00 815 1.00
$90 1363 0.74 (0.66-0.83) P .0001 1331 0.87 (0.79-0.97) P 5.009
Durie-Salmon stage at diagnosis
I 228 1.00 P .0001 222 1.00 P .0001
II 663 1.13 (0.89-1.44) P 5.32 652 1.12 (0.93-1.36) P 5.23
III 1304 1.67 (1.34-2.09) P .0001 1272 1.49 (1.25-1.79) P .0001
Number of lines of chemotherapy‡
1 1292 1.00 P .0001 1256 1.00 P 5.0002
2 635 1.10 (0.96-1.27) P 5.17 628 1.13 (1.00-1.27) P 5.04
2 268 1.66 (1.37-2.01) P .0001 262 1.41 (1.19-1.67) P .0001
Sensitivity to chemotherapy prior to transplant
Other 533 1.00 522 1.00
Sensitive 1662 0.82 (0.72-0.94) P 5.003 1624 0.76 (0.68-0.85) P .0001
Time from diagnosis to transplant
12 months 1554 1.00 1519 1.00
$12 months 641 1.16 (1.01-1.34) P 5.04 627 1.16 (1.03-1.31) P 5.01
RR indicates relative risk.
‡Excludes stem cell priming.
similar median survival (32 and 30 months, respec- comparative study that included 38 Black and 32
tively). There were no differences by stage or MM sub- White AHCT recipients, found that Black patients
type. A smaller study from the Department of Defense had more prolonged responses and greater event-free
equal access health care system, reported on the out- survival (EFS).
comes of 36 Black and 55 White newly diagnosed pa- Unfortunately, there is ample evidence that Blacks
tients receiving AHCT for MM and observed are less likely to receive chemotherapy for MM as well
comparable outcomes between the 2 groups [27]. In as AHCT. Rohatgi et al. [25] reviewed patterns of
their study, there were no differences in the stage, he- chemotherapy use for patients with MM outside the
moglobin, calcium, or creatinine levels, although clinical trial setting. From a population-based retro-
Blacks did have higher C-reactive protein (CRP) levels spective cohort of 49,021 patients aged 65 years or
and a trend for less skeletal involvement. The authors older with stage II or III MM, they found that only
recommended a larger retrospective study such as the 52% received chemotherapy. Blacks were less likely to
current one. Other single center analyses comparing receive chemotherapy compared to Whites (47.6%
Black and White recipients of AHCT for MM have versus 52.8%) despite evidence that use of chemother-
drawn conflicting conclusions. Khaled et al. [28] ana- apy decreased all cause mortality, myeloma specific
lyzed 101 Black patients and concluded that they mortality, and increased survival [25]. The reasons
were likely to relapse earlier after AHCT. Survival for the disparate access are unclear, because control-
was not compared in this study. Saraf et al. [24] in their ling for socioeconomic status did not eliminate the dis-
parity in the receipt of chemotherapy.
These disparities in the receipt of therapy occur in
the transplant setting as well. Joshua et al. [19], in a
previous study from the CIBMTR, demonstrate that
Whites are more likely to receive AHCT for newly
diagnosed MM compared to an age- and sex-adjusted
Black population. Using data from the SEER and
CIBMTR registries, the study showed that age- and
sex-adjusted odds of receiving AHCT for MM is 1.72
times greater in Whites compared to Blacks. Although
our study cannot address the reasons for this underuti-
lization of AHCT in Blacks, interesting conclusions can
Figure 4. Probability of overall survival. be drawn regarding AHCT for MM in Black patients.
20. Biol Blood Marrow Transplant 16:395-402, 2010 Race and Outcomes of AHCT for MM 401
It has been proposed that reduced access to treat- Infectious Diseases (NIAID); a Grant/Cooperative
ment for MM may be related to actual or perceived Agreement 5U01HL069294 from NHLBI and NCI;
worse outcomes in Black patients. Our study clearly a contract HHSH234200637015C with Health
shows that outcomes are not different between Blacks Resources and Services Administration (HRSA/
and Whites receiving AHCT for MM, suggesting this DHHS); 2 Grants N00014-06-1-0704 and N00014-
treatment modality should be offered to all patients 08-1-0058 from the Office of Naval Research; and
when medically appropriate. These results are in ac- grants from AABB; Aetna; American Society for Blood
cordance with a meta-analysis of patients treated for and Marrow Transplantation; Amgen, Inc.; anony-
14 different cancers, where survival in the majority of mous donation to the Medical College of Wisconsin;
cancers was similar between races when comparable Association of Medical Microbiology and Infectious
treatment was given [29]. Disease Canada; Astellas Pharma US, Inc.; Baxter
The pretransplant characteristics of Black recipi- International, Inc.; Bayer HealthCare Pharmaceuti-
ents of AHCT are interesting. The Black cohort was cals; Blood Center of Wisconsin; Blue Cross and
younger and had better performance status than the Blue Shield Association; Bone Marrow Foundation;
White cohort, despite higher rates of anemia and other Canadian Blood and Marrow Transplant Group; Cel-
comorbidities at diagnosis. These differences likely gene Corporation; CellGenix, GmbH; Centers for
indicate a selection bias operating against older Black Disease Control and Prevention; ClinImmune Labs;
patients with lower KPS scores with regard to referral CTI Clinical Trial and Consulting Services; Cubist
for consideration of AHCT. Black patients were also Pharmaceuticals; Cylex Inc.; CytoTherm; DOR Bio-
likely to have had a longer time between diagnosis Pharma, Inc.; Dynal Biotech, an Invitrogen Company;
and transplantation compared to Whites, while receiv- Enzon Pharmaceuticals, Inc.; European Group for
ing a similar number of chemotherapy regimens and Blood and Marrow Transplantation; Gambro BCT,
having similar responses. This suggests delayed refer- Inc.; Gamida Cell, Ltd.; Genzyme Corporation; His-
ral for consideration of AHCT. A referral bias favoring togenetics, Inc.; HKS Medical Information Systems;
only the healthiest Black patients for transplant may be Hospira, Inc.; Infectious Diseases Society of America;
in effect, whereas patients with less favorable clinical Kiadis Pharma; Kirin Brewery Co., Ltd.; Merck
features may only be offered nontransplant or even Company; The Medical College of Wisconsin; MGI
nontreatment options. Pharma, Inc.; Michigan Community Blood Centers;
The major strength of our study is the broad rep- Millennium Pharmaceuticals, Inc.; Miller Pharmacal
resentation of transplant centers making it very likely Group; Milliman USA, Inc.; Miltenyi Biotec, Inc.;
that these results are applicable to the transplant com- National Marrow Donor Program; Nature Publishing
munity as a whole. In this analysis, we are unable to Group; New York Blood Center; Novartis Oncology;
draw any conclusions about factors associated with Oncology Nursing Society; Osiris Therapeutics, Inc.;
nonreceipt of transplant in Blacks because a nontrans- Otsuka Pharmaceutical Development Commercial-
plant population is not represented. The characteris- ization, Inc.; Pall Life Sciences; PDL BioPharma,
tics of the population of black MM patients not Inc; Pfizer Inc; Pharmion Corporation; Saladax
receiving AHCT need to be analyzed to identify the Biomedical, Inc.; Schering Plough Corporation; Soci-
causes of a under utilization of AHCT. It is possible ety for Healthcare Epidemiology of America; Stem-
that many Blacks who are not receiving stem cell trans- Cyte, Inc.; StemSoft Software, Inc.; Sysmex; Teva
plantation for myeloma are forgoing the transplant by Pharmaceutical Industries; The Marrow Foundation;
choice. However, it is also possible that referral bias, THERAKOS, Inc.; Vidacare Corporation; Vion Phar-
unequal access to tertiary care, compliance gap, reluc- maceuticals, Inc.; ViraCor Laboratories; ViroPharma,
tance to enter clinical trials, and socioeconomic dispar- Inc.; and Wellpoint, Inc.
ities account for some of the differences in utilization The views expressed in this article do not reflect
of AHCT for patients with MM. With the demonstra- the official policy or position of the National Institutes
tion of equal outcomes for Blacks with MM, further of Health, the Department of the Navy, the Depart-
study and definitive action to ensure better awareness ment of Defense, or any other agency of the U.S.
and delivery of transplant options for the Black popu- Government.
lation is warranted.
REFERENCES
ACKNOWLEDGMENTS 1. Kyle RA, Rajkumar SV. Epidemiology of the plasma-cell disor-
ders. Best Pract Res Clin Haematol. 2007;20:637-664.
Financial disclosure: The CIBMTR is supported by 2. Kumar SK, Rajkumar SV, Dispenzieri A, et al. Improved survival
Public Health Service Grant/Cooperative Agreement in multiple myeloma and the impact of novel therapies. Blood.
2008;111:2516-2520.
U24-CA76518 from the National Cancer Institute 3. Brown LM, Gridley G, Check D, Landgren O. Risk of multiple
(NCI), the National Heart, Lung and Blood Institute myeloma and monoclonal gammopathy of undetermined signif-
(NHLBI), and the National Institute of Allergy and icance among white and black male United States veterans with