• One ofthe most devastating clinical
manifestation of EPTB.
• 5-1Oo/o of extra-pulmonary & I% of all TB cases.
• Male predominance
• The case fatality rate is 1OOo/o on untreated
case and delayed in treat1nent may lead to
permanent neurological damage.
Introduction
Etiology
►Causative agent;
• Most- Mycobacteriu1n tt1bcrct1losis
• In im1nunoco1nro1nised
patient -
Atypical Mycobacteria ;
MAC, n1ycobacterit1111
intraccl
lt1larc
►Risk factors;
Children> adults
HIV co-infection
Malnutrition
• Alcoholics
• Malignacies
Use of
• •
Immnosuppressive
agents
7.
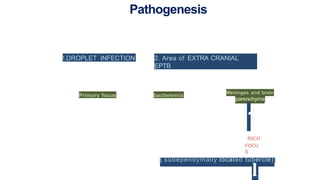
Pathogenesis
!.DROPLET INFECTION 2.Area of EXTRA CRANIAL
EPTB
Primary focus bacteremia
Meninges and brain
parenchyma
1
RICH
FOCU
S
( subependymally located tubercle)
l
Staging of TBM
BritishMedical Research Council criteria
Stage I: Prodro1nal phase with no definite neurologic
sy1nptoms.
Stage II: Signs of n1eni11geal irritation with slight or no
clouding of sensorium & minor or no
neurological deficit.
Stage III: Severe clouding ofsensorium, convulsions, focal
neurological deficit & involuntary 1nove1nents.
13.
Modified MRC criteria
GradeI: Alert and oriented (GCS 15) without focal
neurological deficit.
Grade II: GCS 14-10 with or without focal neurological
deficit or GCS 15 with focal neurological deficit.
Grade Ill: GCS less than 10 with or without focal
neurological deficit.
14.
Spinal
TBM
May result fromruptt1re of Rich foci in the spinal
aracl1noid
space
The acute form presents with fever, headache, and root pains
acco1npanied by myelopathy
The chro11ic form presents with spinal cord compression
• One ofthe most devastating clinical
manifestation of EPTB.
• 5-1Oo/o of extra-pulmonary & I% of all TB cases.
• Male predominance
• The case fatality rate is 1OOo/o on untreated
case and delayed in treat1nent may lead to
permanent neurological damage.
Introduction


























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




