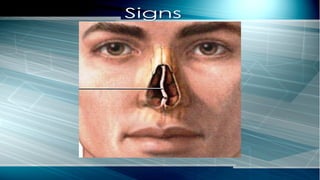
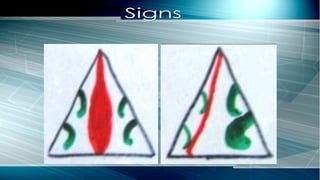
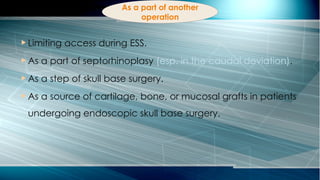
The document discusses the classification of septal deviations and their implications for surgery, highlighting various types and associated symptoms, as well as indications for surgical intervention. It emphasizes the need for careful consideration before performing septoplasty, particularly in children, and the controversies surrounding techniques, postoperative care, and antibiotic use. Ultimately, the document advocates for advancing surgical practices to effectively correct deviations while minimizing complications.