Downloaded 15 times
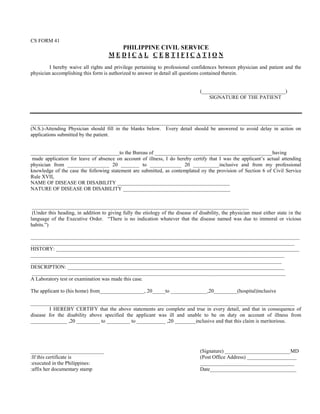

This document is a medical certification form completed by a physician to certify a patient's illness and request for leave of absence. The form contains sections for the physician to provide details such as the name and nature of the disease/disability, history, description, results of any laboratory tests, dates the patient was unable to work or in the hospital due to illness, and a certification that the physician's statements are true and the leave request is merited. The patient also provides a waiver at the top authorizing the physician to disclose medical details to answer the questions on the form.