
Recommended
Recommended
More Related Content
Similar to Critiquing Evaluation Criteria for Quantitative Research Artic
Similar to Critiquing Evaluation Criteria for Quantitative Research Artic (20)
More from MargenePurnell14
More from MargenePurnell14 (20)
Recently uploaded
Recently uploaded (20)
Critiquing Evaluation Criteria for Quantitative Research Artic
- 1. Critiquing Evaluation Criteria for Quantitative Research Article Listed below are criteria that you will use to critique research articles pertinent to your research area of interest. Discuss how the investigator satisfied each criterion. Cite relevant passages in the articles, with reference to page number if appropriate. Don’t merely respond “yes” or “no” to the presence or absence of each criterion – you must provide examples and rationale for your response. Criteria YES NO Comments I- Title of the Article and Authors Is the title clear, including area of study and group studied? Are the author’s credentials included? II- Introduction Is the purpose of the study presented? Is the significance (importance) of the problem discussed? Does the investigator provide a sense of what he or she is doing and why? III- Problems Statement Is the problem statement clear? Does the investigator identify key research questions and variables to be examined?
- 2. Does the study have the potential to help solve a problem that is currently faced in clinical practice? IV- Literature Review Does the literature review follow a logical sequence leading to a critical review of supporting and conflicting prior work? Is the relationship of the study to previous research clear? Does the study have the potential gaps in the literature and support the necessity of the present study? V- Theoretical Framework and Hypotheses Is a rationale stated for the theoretical/conceptual framework? Does the investigator clearly state the theoretical basis for hypotheses formulation? Is the hypotheses stated precisely and in a form that permits it to be rested? VI- Methodology Are the relevant variables and concepts clearly and operationally defined? Is the design appropriate for the research questions or hypotheses? Criteria YES NO Comments
- 3. Are methods of data collection sufficiently described? What are the identified and potential threats to internal and external validity that were present in the study? If there was more than one data collector, was interrater reliability adequate? VII- Sample Are the subjects and sampling methods described? Is the sample of sufficient size for the study, given the number of variables and design? Is the adequate assurance that the rights of human subjects were protected? VIII- Instruments Are appropriate instruments for data collection used? Are reliability and validity of the measurement instruments adequate? IX- Data Analysis Are the statistical tests used identified and the values reported? Are appropriate statistics used, according to level of measurement, sample size, sampling method, and hypotheses/research questions? X- Results Are the results for each hypothesis clearly and objectively presented? Do the figures and tables illuminate the presentation of results?
- 4. Are results described in light of the theoretical framework and supporting literature? XI- Conclusion/Discussion Are conclusions based on the results and related to the hypotheses? Are study limitations identified? Are implications of findings discussed (i.e., for practice, education, and research)? Are recommendations for further research stated? XII- Research Utilization Implications Is the study of sufficient quality to meet the criterion of scientific merit? Does the study meet the criterion of replicability? Is the study of relevance to practice? Do the benefits of the study outweigh the risks? XIII- Format Utilizes APA format Includes the list of references utilizing APA
- 5. Depression among patients with end-stage renal disease in hemodialysis Geraldo B. Silva Juniora,b,c*, Elizabeth F. Daherb, Ana Paula A. Buosid, Rafael S.A. Limac, Mikaelly M. Limac, Eveline C. Silvac, Aline M. Sampaiob, João Moisés L. Santanac, Francisco Emmanuel C. Monteiroc and Sônia M.H.A. Araújoa aSchool of Medicine, University of Fortaleza, Fortaleza, Brazil; bDepartment of Internal Medicine, School of Medicine, Federal University of Ceará, Fortaleza, Brazil; cCentro de Nefrologia de Caucaia, Caucaia, Brazil; dSchool of Psychology, State University of Ceara, Fortaleza, Brazil (Received 28 May 2013; accepted 12 September 2013) Depression is frequent in end-stage renal disease (ESRD) and predicts mortality in dialysis patients. The aim of this study was to investigate the occurrence of depression among patients on hemodialysis. We conducted an observational cross- sectional study at two hemodialysis centres in the metropolitan area of Fortaleza, Ceará, Brazil, between September and October 2010. The occurrence of depression was evaluated according to Beck Depression Inventory II. Among 148 patients interviewed, the mean age was 46 ± 13 years and 54% were male. The average
- 6. time on dialysis was 5.3 ± 5.2 years. Depression was found in 101 (68.2%) cases. Depression was classified as mild (49.5%), moderate (41.5%) and severe (9%). Only 15.5% had prior depression diagnosis. Follow-up with Psychologist was being done in only 32.4% of cases. Patients with depression had a higher frequency of antidepressant use (20.7% vs. 4.2%, p = .01) and benzodiazepines (33.6% vs. 8.5%, p = .001). Among patients using antidepressant, improvement of symptoms was reported by 81.6%. Depression is one potentially modifiable risk factor in ESRD. The investigation and multidisciplinary approach of depression should be part of routine evaluation of patients on dialysis. Keywords: depression; chronic kidney disease; end-stage renal disease; hemodialysis Introduction Chronic kidney disease (CKD) and its treatment represent a major stress for the affected individuals and, frequently, require considerable social adaptation. There are many factors reported to be associated with health-related quality of life including age, gender, education, income, comorbid conditions, hemoglobin level, personality characteristics, depression, anxiety and others (Franke, Reimer, Philipp, & Heemann, 2003; Matas et al., 2002; Prihodova et al., 2009). The prevalence of depression is higher in end-stage renal
- 7. disease (ESRD) patients than in the general populations (Chilcot, Wellsted, Da Silva- Gane, & Farrington, 2008) and predicts mortality in dialysis patients (Riezebos, Nauta, Honig, Dekker, & Siegert, 2010). The aim of this study is to investigate the occurrence of depression among patients with CKD on hemodialysis. *Corresponding author. Email: [email protected] © 2013 Taylor & Francis Psychology, Health & Medicine, 2014 Vol. 19, No. 5, 547–551, http://dx.doi.org/10.1080/13548506.2013.845303 mailto:[email protected] http://dx.doi.org/10.1080/13548506.2013.845303 Methods This was an observational cross-sectional study conducted at two hemodialysis centres in the metropolitan area of Fortaleza, Ceará, Brazil, between September and October 2010. The Beck Depression Inventory II (BDI-II) questionnaire consisting of 21 items was administered as a diagnostic tool (Beck, Ward, Mendelson, Mock, & Erbaugh, 1961). A signed consent was obtained before filling out the forms. Depression was classified as mild (score 10–18), moderate (score 19–29) and severe (score >30). The study protocol was reviewed and approved by the Ethics Committee of the University of Fortaleza.
- 8. Statistical analysis was performed using Epi Info, version 6.04b. The comparison between two groups of patients (depression vs. non-depression) was done using Student’s t-test, Fischer exact test, Mann–Whitney test and Chi-square test when appropriate. “p values” below 5% ( p < .05) were considered statistically significant. Results A total of 180 patients were interviewed, of which 148 accepted in answer the question- naire. The mean age was 46 ± 13 years and 54% were male. The average time on dialy- sis was 5.3 ± 5.2 years. Depression was found in 101 (68.2%) cases. The intensity of depression was classified as mild in 50 (49.5%), moderate in 42 (41.5%) and severe in 9 (9%) patients. Only 23 patients (15.5%) had prior depressive diagnosis. Follow-up with Psychologist was being done in only 48 cases (32.4%). Comparison between patients with and without depression showed similar age (45.2 ± 14 years vs. 48.2 ± 12.9 years, p = .21), gender (male 53.4% vs. female 55.3%, p = .86) and time on dialysis (5.5 ± 5.2 vs. 4.9 ± 5.1 years, p = .51) (Table 1). Patients with depression had a higher frequency of antidepressant use (20.7% vs. 4.2%, p = .01) and benzodiazepi nes (33.6% vs. 8.5%, p = .001). Among 46 (86.9%) patients who were using antidepressant, improvement of symptoms was reported by 40 (81.6%) patients. A comparison between
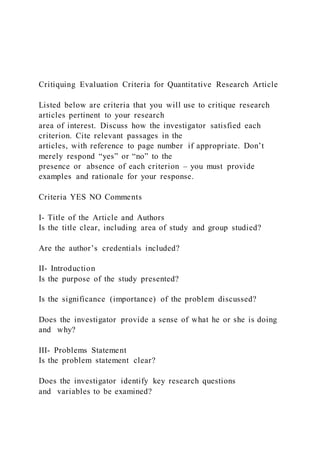
- 9. Table 1. Comparison of depression and non-depression in patients with ESRD in hemodialysis. Parameter Depression (n = 101) Non-depression (n = 47) p Age (years) 45.2 ± 14.0 48.2 ± 12.9 .21 Gender Male 54 (53.4%) 26 (55.3%) .86 Female 47 (46.6%) 21 (44.7%) .10 Employment 33 (32.6%) 22 (46.8%) .10 Time on dialysis (years) 5.5 ± 5.2 4.9 ± 5.1 .51 Previous kidney transplantation 7 (6.9%) 6 (12.7%) .34 Preparing to kidney transplantation 40 (39.6%) 23 (48.9%) .29 BDI-II score 19.4 ± 7.8 5.5 ± 2.6 .0001 Use of antidepressant 21 (20.7%) 2 (4.2%) .01 Use of benzodiazepines 34 (33.6%) 4 (8.5%) .001 Improvement with medication 40 (39.6%) 6 (12.7%) .001 Psychologist follow-up 36 (35.6%) 12 (25.5%) .26 Family history of depression 28 (27.7%) 10 (21.2%) .54 Low income 79 (78.2%) 41 (87.2%) .26 Family support 76 (75.2%) 41 (87.2%) .12 Smoking 8 (7.9%) 2 (4.2%) .50 Alcoholism 7 (6.9%) 4 (8.5%) .74 Physical activity 27 (26.7%) 15 (31.9%) .55 Notes: BDI-II = Beck Depression Inventory II. Values expressed as mean ± SD. Student’s t-test and Fisher exact test. Significant p < .05. 548 G.B. Silva Junior et al. patients with moderate to severe depression and patients without depression is shown in
- 10. Table 2. Discussion Depression is widely recognized as the most common psychiatric problem in patients with ESRD and is considered the second most common medical problem in this popula- tion after hypertension (Chilcot et al., 2008). Depression has been associated with lack of adherence to treatment, suicidal tendencies and poor survival rates (Diefenthaeler, Wagner, Poli-de-Figueiredo, Zimmermann, & Saitovitch, 2008). It is important to consider that complaints of malaise, anorexia and sleep disturbances can be mistaken for depressive symptoms (Murtagh, Addington-Hall, & Higginson, 2007). Chilcot, Davenport, Wellsted, Firth, and Farrington (2011) found significant depressive symptoms (BDI-II score ≥ 16) in 25% of hemodialysis patients. In the present study, depression was found in 68% of cases, which is impressive high. Most studies performed worldwide report increased depressive symptoms in females (Araújo et al., 2012; Saeed, Ahmad, Shakoor, Ghafoor, & Kanwal, 2012). In the present study, the majority of depressed patients (54%) were male. According to another study (Chilcot et al., 2011), only 15% of depressed patients had prior depressive diagnosis. Despite the high incidence of depression in dialysis patients, the diagnosis is often
- 11. missed and not addressed, focusing only on the physical aspects of the disease (Cukor, Cohen, Peterson, & Kimmel, 2007). Saeed et al. (2012) found moderate and severe depression in 75% of studied cases. In the present study, only 15% had prior depressive diagnosis. The intensity of depression was classified as mild in 50%, moderate in 41% and severe in 9% of patients. Employment status of an individual was associated with higher frequency of depres- sion (Saeed et al., 2012). In our patients with depression, 67% were unemployed and 78% had low income level, but there were no statistical difference between depressive Table 2. Comparison of moderate-severe depression and non depression in patients with ESRD in hemodialysis. Moderate-severe depression (n = 55) Non-depression (n = 47) p Age (years) 45.5 ± 14.1 48.2 ± 12.9 .26 Gender Male 29 (52.7%) 26 (55.3%) .83 Female 26 (47.3%) 21 (44.7%) Employment 33 (60%) 22 (46.8%) .52 BDI-II score 22 ± 6.8 5.5 ± 2.6 .0001 Time on dialysis (years) 6.2 ± 6.0 4.9 ± 5.1 .40 Previous transplantation 5 (9.0%) 6 (12.7%) 1.0 In preparation for transplantation 22 (40%) 23 (48.9%) .40
- 12. Family support 42 (76.3%) 41 (87.2%) .19 Use of medication 28 (51%) 6 (12.7%) .0001 Use of antidepressant 11 (20%) 2 (4.2%) .06 Use of benzodiazepine 21 (38%) 4 (8.5%) .0001 Psychologic follow-up 23 (41.8%) 12 (25.5%) .28 Improvement with medication 22 (78.5%) 6 (12.7%) .005 Notes: Values expressed as mean ± SD. Student’ s t-test and Fisher exact test. Significant p < .05. Psychology, Health & Medicine 549 and non-depressive group, maybe due to the high prevalence of unemployment and low income. There is mixed evidence that treating depression has a positive impact on survival outcomes in other physical illnesses (Detweiler-Bedell, Friedman, Leventhal, Miller, & Leventhal, 2008). The use of antidepressants is reported to be as low as 10% (Chilcot et al., 2011). In the present study, only 20% of patients with depression were using antidepressant and 33% benzodiazepines. Among patients using antidepressant, 82% reported improvement of symptoms. In summary, depression is one potentially modifiable risk factor that is associated with high mortality and non-adherence among patients in dialysis. Depression is a frequent and underdiagnosed disease in these patients. Follow - up with a Psychologist is
- 13. also uncommon, as well as the specific drug treatment. The investigation of depression should be part of routine monitoring of patients on dialysis. Multidisciplinary approach needs to be sought in treating dialysis patients involving Psychologists, Psychiatrists and Nephrologists to improve the quality of life in these patients. Study limitations There are some limitations in this study. The number of patients could be higher, but it is difficult to convince all patients of our centre to enrol the study. The cut-off values used in the questionnaire may overestimate the prevalence of depression. There are also other approach methods to assess depression in these patients. References Araújo, S.M., de Bruin, V.M., Daher E.de F., Almeida, G.H., Medeiros, C.A., & de Bruin, P.F. (2012). Risk factors for depressive symptoms in a large population on chronic hemodialysis. International Urology and Nephrology, 44, 1229–1235. Beck, A.T., Ward, C.H., Mendelson, M., Mock, J., & Erbaugh, J. (1961). An inventory for mea- suring depression. Archives of General Psychiatry, 4, 561–571. Chilcot, J., Davenport, A., Wellsted, D., Firth, J., & Farrington, K. (2011). An association between depressive symptoms and survival in incident dialysis patients. Nephrology Dialysis Trans- plantation, 26, 1628–1634.
- 14. Chilcot, J., Wellsted, D., Da Silva-Gane, M., & Farrington, K. (2008). Depression on dialysis. Nephron Clinical Practice, 108, c256–c264. Cukor, D., Cohen, S.D., Peterson, R.A., & Kimmel, P.L. (2007). Psychosocial aspects of chronic disease: ESRD as a paradigmatic illness. Journal of the American Society of Nephrology, 18, 3042–3055. Detweiler-Bedell, J.B., Friedman, M.A., Leventhal, H., Miller, I.W., & Leventhal, E.A. (2008). Integrating co-morbid depression and chronic physical disease management: Identifying and resolving failures in self-regulation. Clinical Psychology Review, 28, 1426–1446. Diefenthaeler, E.C., Wagner, M.B., Poli-de-Figueiredo, C.E., Zimmermann, P.R., & Saitovitch, D. (2008). Is depression a risk factor for mortality in chronic hemodialysis patients? Revista Brasileira de Psiquiatria, 30, 99–103. Franke, G.H., Reimer, J., Philipp, T., & Heemann, U. (2003). Aspects of quality of life through end-stage renal disease. Quality of Life Research, 12, 103–115. Matas, A.J., Halbert, R.J., Barr, M.L., Helderman, J.H., Hricik, D.E., Pirsch, J.D., ... Ferguson, R.M. (2002). Life satisfaction and adverse effects in renal transplant recipients: A longitudinal analysis. Clinical Transplantation, 16, 113–121. Murtagh, F.E., Addington-Hall, J., & Higginson, I.J. (2007). The prevalence of symptoms in end-
- 15. stage renal disease: A systematic review. Advances in Chronic Kidney Disease, 14, 82–99. Prihodova, L., Nagyova, I., Rosenberger, J., Roland, R., van Dijk, J.P., & Groothoff, J.W. (2009). Impact of personality and psychological distress on health- related quality of life in kidney transplant recipients. Transplant International, 23, 484–492. 550 G.B. Silva Junior et al. Riezebos, R.K., Nauta, K.J., Honig, A., Dekker, F.W., & Siegert, C.E. (2010). The association of depressive symptoms with survival in a Dutch cohort of patients with end-stage renal disease. Nephrology Dialysis Transplantation, 25, 231–236. Saeed, Z., Ahmad, A.M., Shakoor, A., Ghafoor, F., & Kanwal, S. (2012). Depression in patients on hemodialysis and their caregivers. Saudi Journal of Kidney Diseases and Transplantation, 23, 946–952. Psychology, Health & Medicine 551 Copyright of Psychology, Health & Medicine is the property of Routledge and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use.
- 16. Abstract Introduction Methods Results Discussion Study limitationsReferences