Download to read offline



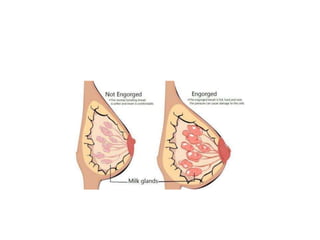


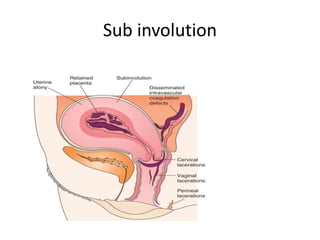





















This document discusses various nipple and breast disorders that can occur postpartum, including inverted nipples, cracked nipples, mastitis, breast engorgement, breast abscesses, and subinvolution of the uterus. It describes the grades of nipple inversion, treatments for inverted nipples like Hoffman's technique and piercings. It also discusses causes, signs, and treatments for conditions like cracked nipples, mastitis, breast engorgement, and breast abscesses. Surgical and antibiotic treatments for issues like wound abscesses, hematomas, and pelvic abscesses are also summarized.















































