INTRODUCTION
Mental health professionalspractice within the framework of a conception model
It is an organized complex body of knowledge such as concepts related to human
behaviour
The conceptual model provides philosophical fragments orientations to the
services and scientific knowledge of rendering better services responsibilities and
accountability
The recognized conceptual models that are used in psychiatric nursing practice or
interpersonal model existential model behaviour model psychoanalytical model
3.
DEFINITION
It convince thegeneral meaning of the concepts in
a manners that fits the theory it also describe the
activity necessary to measure the constructs
relationships or variables within a theory
-K.P. Neeraja
Basic Assumptions ofInterpersonal Theory
Human being is a social being he is behaviour grows
out of his attempts to establish a meaningful social
relationship with others
Human beings are having the capacity to live
effectively in relationship with others
Personality development is determined in the context
of social interactions with others and it is influenced by
both biological and social factors
7.
Sublimation
It is anunconscious process made by
socially acceptable behavioural patterns or
substituted to satisfy partially the needs for
a behavioural pattern
8.
Selective in Attention
Itis an unconscious substitute process
which cause anxiety go unnoticed by
the individual
9.
Dissociation
It will beused to buy an individual
unconsciously to minimise parts of the
individuals experience is to avoid
anxiety
10.
Basic Principles ofInterpersonal Theory
Development proceeds through various stages in
each states there is involvement of different patterns
of relationship
For example, in infancy need for contact us full field
by the parents
11.
Basic Principles ofInterpersonal Theory (Conti…)
a. In childhood:
Active participation in activities and interaction with adults will be observed
b. In pre adolescent and adolescent:
Detachment from parents and attachment with peer group increases
c. In early adulthood:
Intimate relationship with Hetero sexual groups resulting into marriage and
family formation
If any failure to make progress satisfactory through various stages may result into
maladapt to behaviour
12.
Basic Principles ofInterpersonal Theory (Conti…)
d. Anxiety:
It has a direct relationship with the personality formation
For example, for fulfilment of basic needs, an Infant will
depend on a caretaker
e. Early life experience:
Attachment to caretakers to the Infant especially the mother
will influence the individual’s development throughout his life
13.
Basic Principles ofInterpersonal Theory (Conti…)
f. Social exchange:
The social relationship is established to meet mutual needs each person
needs mutual helper recognition from others for self-identification
g. Social roles:
Every individual has to perform a specific social role said by society
example teacher mother
h. Interpersonal accommodation:
To our more persons interact with each other and establish certain goals to
build a satisfying relationship
14.
Modes in CognitiveProcess
1. Prototyxic mode
It is characterized by sensations, feelings
2. Para taxic mode
It is also illogical in nature that simultaneous events are considered as
casually related
3. Syntaxic mode
It is developed form characterised by logical thinking emergences in the
Juvenile stage individual develops the ability to relate effectively through this
mode
Human development process through stages of development from infancy
to toddler stage according to Biplo nursing is an interpersonal process that
makes the basic needs of an individual and maintains health status
Role of thePatient and the Interpersonal Therapist
In this model that therapist act as participant and
observer he is role is to activity engage the patient
The therapist will have balanced values 3rd and
feelings and interacts as a real person
17.
Application to Nursing
Interpersonaltheory has been occupied
cornerstone in psychiatric nursing concepts
like anxiety trust securities selfie stick
Anders client relationship
18.
Dimensional Approach
a) Unityof interaction
b) Dimensions of interpersonal behaviour focus
c) Interdependency
d) Affiliation
e) Patterns of dyadic interaction
(It is stabilized into a characteristic patterns of interpersonal behaviour)
Introduction
Segment Freud explainedthe theories of the mind, the
subsequent work by Eric Erikson has greatly added and
changed many of the initial concepts
Psycho analysis system was presented on both theoretical
and practical side on the theoretical side
It presented a theory to understand and explain the human
psyche on the practical side
It studies human behavior and also a therapy to treat the
mentally ill patient
21.
DEFINITION
A psychological theoryof mind and personality
development based primarily on concept of
intracystic conflict
-K.P. Neeraja
22.
Basic Concepts
1. Psychicenergy is psychic determinism:
All mental activities conscious and unconscious process meaningful and
purposeful activities that are connected with previous life experiences.
2. Drives:
The motivating forces that determine the behavior of an individual originate from
bio-somatic processes and or are experienced as wishes
3. Cathexis:
The concentration of mental energy on one particular person Idea or object
4. Anti cathexis:
Diversion of mental energy the urging forces are to satisfy
23.
Theories of Mindor Topography Theory of Mind
Introduction
According to this theory, the mind structure of
the human psyche is divided into 3 layers.
This theory was developed by Sigmund Freud in
1900
24.
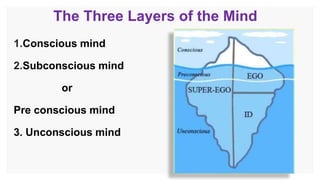
The Three Layersof the Mind
1.Conscious mind
2.Subconscious mind
or
Pre conscious mind
3. Unconscious mind
25.
The Three Layersof the Mind
1. Conscious mind:
Conscious mind upper portion of the mind
The conscious mental process of thinking is based on the
reality principle
It is a special sense and the cone of attention comes
underwear registration of stimulate from both within
internal and outside
26.
2. Subconscious mindor Pre conscious mind:
It stores all types of information just the surface of
awareness
It can be easily brought to the level of conscious ATM
moments notice whenever required all experience is or
knowledge which have been gained or learned by an
individual through various types of experiences are training
It is between the unconscious mind and the conscious mind
27.
3. Unconscious mind:
Theunconscious mind contains ideas and effects
that repress material wishes, designs, feelings, and
motives that can only reach the conscious through
precious than the conscious mind is based on the
pleasure principle id
Anal Phase (1-3Years)
The child gets gratification through the anal and perianal
areas a major achievement in this stage
Annual sphincter control is achieved through toilet training
It consists of two phases
The first one is anal erotic face excretion
The second one is anal sadistic face holding
30.
Oedipal or PhallicPhase (3 to 5 years)
The odipose complex includes the wish of
the child for an exclusive libidinal
relationship with the parent of the opposite
sex
31.
Latency Phase (5to 12 years)
This is a stage of relatives’ actual superheroes are
formulated.
Socially appropriate girls like the development of
social interpersonal relationships knowledge and
new skills engage in economic and socialization
activities
32.
Genital Phase (12to 18 years)
It is associated with no neuroendocrine and
bio-somatic maturational components as
adults develops children will develop the
capacity for intimacy and respect for
others
33.
The Structural Theoryof Mind
In 1923 Sigmund Freud divided the
mental operators into three dynamic
components id, ego, and superego
from the structural theory of mind
1. Id:
It isunconscious containing the basic drives
It has the qualities like it must get what it wants and when
it wants in this way it is quite selfish and unethical
It is characterized by the primary process of thinking and is
based on the pleasure principle lacking direct contact with
reality.
It will not follow any rules and consider only satisfaction of
its phone needs and drives
36.
2. Ego:
The egois primarily determined and guided by the
reality principle
It is intermediate between three sides of forces
The ego maintains a balance between the Id and
superego
Ego is the seat of conscious intellectual differences
function of the mental apparatus
37.
3. Superego:
It isa predominantly unconscious
subdivision of mental operators from the
ego it is the direct and the antithesis of the
id and represents the ethical and moral
aspects of the psyche
Introduction
It is deliveredfrom learning theories focused on
clients’ actions not on thoughts and feelings
behavioural approach is used frequently to
control the undesirable behaviour
40.
Techniques of BehaviourTherapy
Systematic Desensitization – Indication: Phobia obsessive
compulsive neurosis anxiety
This technique is based on the receive approval inhibition behavioural
principle of Counter conditioning in this clients will attain complete
relaxation and or then be exposed to the stimulus
Relaxation training will be given example meditation mental imaginary
Ask the client to construct a hierarchy of anxiety
Desensitization of the stimuli patient is asked to give a signal
whatever anxiety is produced with each signal He is asked to relax
41.
Operant conditioning proceduresto increase adaptive
behaviour
Positive reinforcement - to rain force or improve the
performance of the desirable behavior repeatedly a token or
reward material or symbolic appreciation will be given
whenever the client performs an acceptable behavior
Token economy
Chronically hospitalized patients children up to adolescent
age it is a positive reinforced program
42.
Operant conditioning processorto teach new behaviour
1. Modelling:
New desirable behaviour through imitation are by demonstration the client
will be allowed to observe
2. Shaping:
The therapist tries to shape the decided behavioural skills step by step he
positively reinforces the existing behavior and the response
3. Chaining:
Training will be given to learn the complete task in a break up manner
step by step forward chaining and backward chaining.
43.
Operant conditioning processorto teach new behaviour (Conti…)
4. Forward chaining:
The therapist will identify the difficulty of the client in performing complex task he will
give chaining to the client to learn first step second step client will achieve third step
until achieve the task
5. Backward Chaining:
In backward direction step by step the client will be assisted to learn desirable task from
last step to next step
6. Backward Chaining:
In backward direction step by step the client will be assisted to learn desirable task from
last step to next step
7. Promoting:
Assisting the client to learn specific target behaviour repeatedly insisting the importance
of desired behaviour and make the client to understand and learn it
44.
Operant Conditioning Procedurefor Decreasing
Maladaptive Behaviour
1. Indications: Childhood disorders
2. Time out: If the client forms desirable acts exhibits and desirable behaviour
3. Response cost: To teach adaptive behaviour among the client token
programs were activated
4. Punishment: Whenever desirable behaviour is expected it has to be
avoided by administrating some shorts of punishment with a proper or clear
explanation
5. Ignoring: Whenever the problem Attic behaviour exists rewards or attention
can be removed Example: Not having high eye contact or physical contact
6. Restitution: If the client exhibits and desires are a problem behaviour it will
be corrected by giving a wide range of punishment
45.
Assertiveness Training:
Alleviates interpersonallybased on anxiety
Improve the ability to stand up for one’s rights
Technique:
The therapist will give assertive behaviour training by
role-playing coaching Modelling and role reversal
techniques and then by practicing in it a real life
situations
46.
Aversion Therapy:
Indication -alcoholism smoking
Technique:
When an unpresent response occurs due to pleasurable
stimuli immediate punishment and social disapproval
have to be given the curious of unpleasant response
can be prevented
47.
Flooding:
Indication:
Anxiety, Phobia, Agarphobia, Speaking difficulties
The therapist will provide Guidance counseling
encouragement for the client to face and so it is
situations in a nongraded manner with no attempt to
reduce anxiety
48.
Reciprocal Inhibition:
Wolpe hasdescribed this technique according to
this theory the observable behavior or symptom is
a learned response to anxiety that leads to the
detection of anxiety.
The therapist will instruct the client to express
anxiety
49.
Role of nursein behavioural therapy
Nurses have to keep in mind the principle of
learning while administering behavioral therapy to
the clients
Uses behavioral approaches like positive
reinforcement relaxation techniques involving the
client and the significant people in the provision of
care
Existential View ofBehavioural Deviation
Behaviour deviations will occur
When an individual is not free to choose from
among alternative behaviour
When the individual awards socially acceptable
and responsible behaviour
Role of ExistentialTherapist
Therapist Act as a guide director and role model
Provides warm and caring ki values to the client
Help the client to find his way
56.
Role of theClient
Client is active in therapy
The client must be open and honest ready for
change
Accepts responsibility for his behaviour
57.
Therapies based onthe existential model
1. Reality Therapy:
William Glosser invoked this client is help to
identify the life goals and guide the ways to
accomplish is goals
58.
2. Psycho Synthesis:
Robertoexplained that the self is considered the inner
centre of awareness and peace-guided imagination and
meditation techniques will be used to achieve self-
awareness and control over the course of his life
3. Rational Emotional Therapy:
Creative oriented
59.
4. Therapy Albert:
Theclient is encouraged to accept as he is under to
take rest and challenges to try out a new behavior or
action
5. Gestalt Therapy:
Fredrick S. Peris emphasized it the therapist will
encourage the client to identify the feeling which will
enhance self-awareness, self-acceptance
60.
6. Future-Oriented Therapy:
ViktorE. Frank explains the therapy client is oriented towards the
spiritual meaning of his life logos primary life force helps the client
to become aware of his responsibility is the client is guided to take
control of his own life
7. Encounter Group:
Carl Rogers explains the establishment of intimate interactions in a
group situation the client is expected to assume responsibility for his
behaviour and feelings in stress group exercises are practices