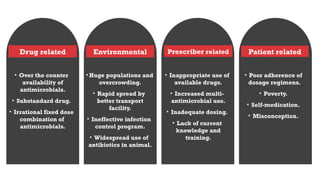
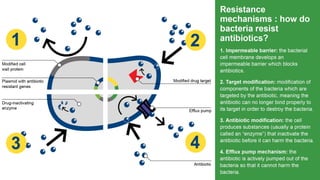
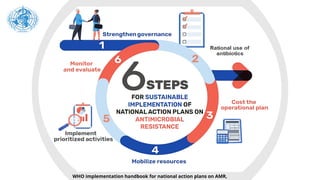
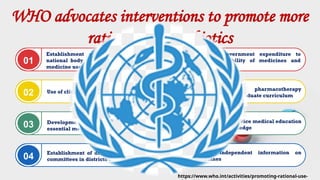
Antimicrobial resistance (AMR) occurs when pathogens resist treatments, complicating infection management and increasing mortality risks. The document outlines contributing factors to AMR such as inappropriate drug use, environmental issues, and patient behaviors, highlighting the global burden of antibiotic resistance, with millions of deaths linked to it. Measures to combat AMR include promoting rational antibiotic use, establishing guidelines, improving healthcare training, and developing new drug therapies.

















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




