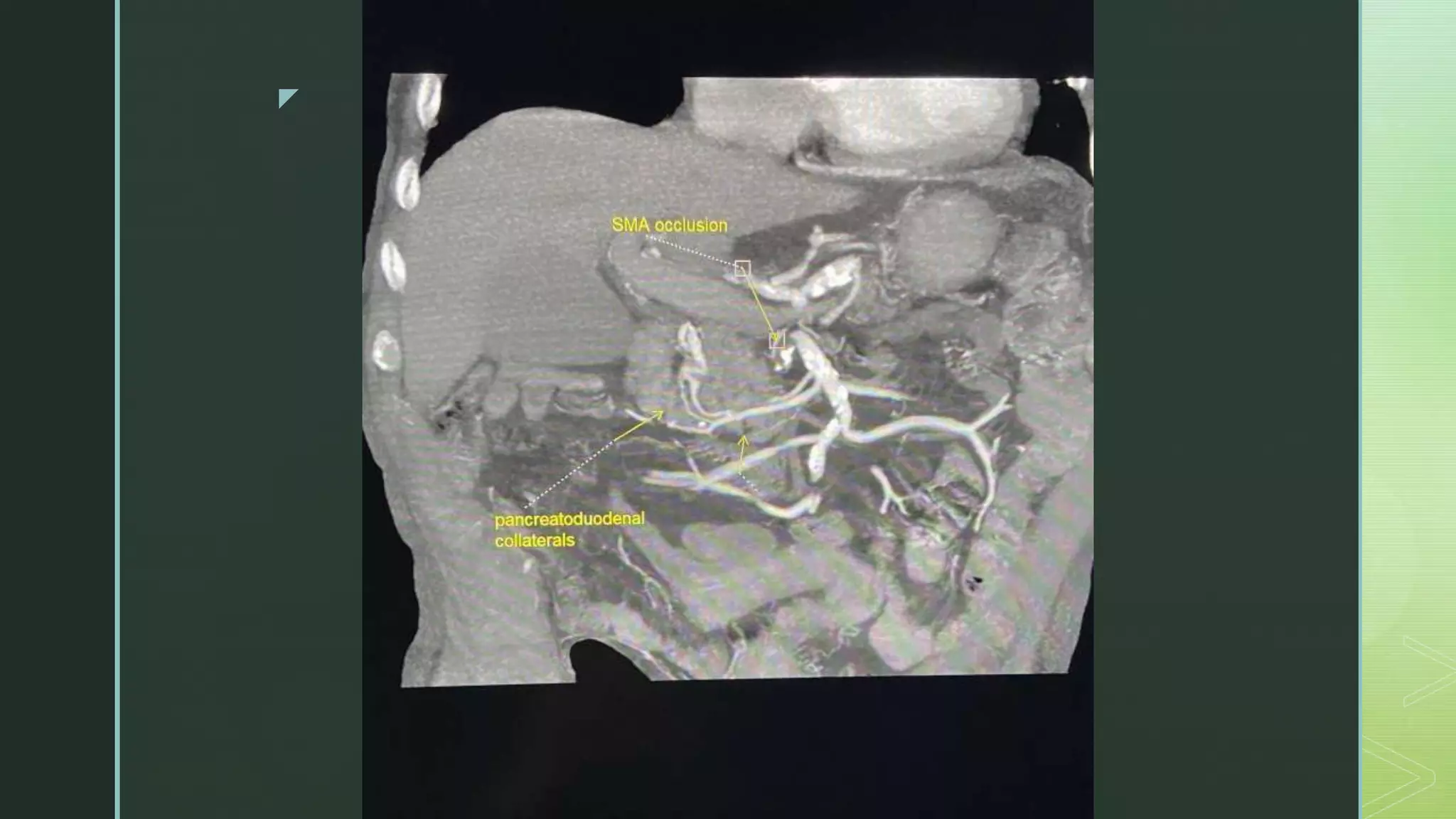
A 78-year-old male presented with abnormal labs showing severe anemia. Further testing revealed mild iron deficiency but no other cause. The patient suffers from chronic mesenteric ischemia likely due to atherosclerotic narrowing of the celiac and superior mesenteric arteries, which is the most common cause. Chronic mesenteric ischemia results in reduced blood flow to the intestines and presents with symptoms like recurrent post-prandial abdominal pain or an adapted eating pattern to avoid pain. CT angiography is the preferred imaging study to diagnose chronic mesenteric ischemia through detection of stenosis in the celiac and superior mesenteric arteries.





![z
ETIOLOGY AND ASSOCIATIONS
Atherosclerosis: The majority of cases of chronic mesenteric
ischemia are caused by atherosclerotic narrowing of the origins
of the celiac or superior mesenteric arteries
Other: Rare causes of chronic mesenteric ischemia include
fibromuscular dysplasia, aortic or mesenteric artery dissection,
vasculitis (polyarteritis nodosum, Takayasu disease [8]), and
retroperitoneal fibrosis](https://image.slidesharecdn.com/chronicmesentericischemiacopy-230120141309-d3af983f/75/Chronic-Mesenteric-Ischemia-8-2048.jpg)