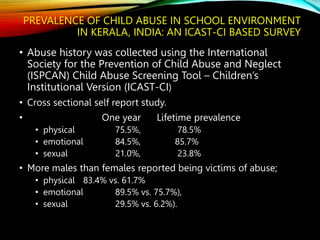
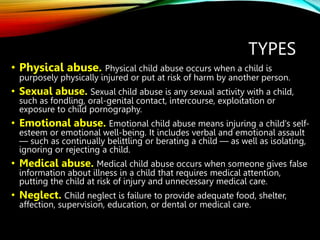
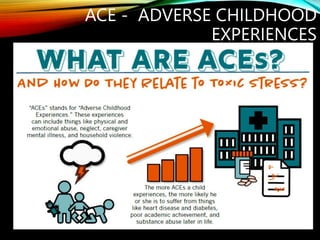
The document discusses child sexual abuse in India. It defines child sexual abuse according to WHO and provides statistics on its prevalence in India, with 18 crore or 1/3 of Indian children estimated to be affected. Studies in Kerala found 36-35% of boys and girls reported sexual abuse by late adolescence. The document also outlines the types of child abuse, signs and symptoms, impact on health and brain, Adverse Childhood Experiences, and the provisions of the Protection of Children from Sexual Offences Act, 2012 in India to prevent child sexual abuse and punish offenders.




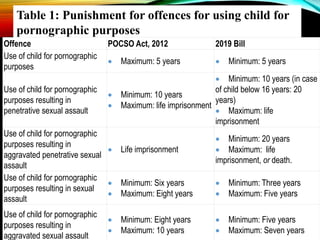
![• The elevated and increased response of catecholamines and
CRF as discussed above can result in mechanisms that cause
accelerated neuronal loss, decreased neuronal size, reduced
number of synapses, abnormalities in developmentally
appropriate pruning, and inhibition of neurogenesis at vital
periods along with inadequate production and expression of
brain-derived neurotrophic factor.[62],[63],[64],[65],[66]](https://image.slidesharecdn.com/childabuseandpocso-230130092514-bb53bb72/85/CHILDABUSE-AND-POCSO-pptx-30-320.jpg)






























![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



