Approach to theChild with
Irritability
Presented by : Mukose Godfrey
Lecturer: Dr. MUNANURA
2.
The outline
• Introduction
•Etiologies
• Clinical presentation
• Investigations
• Differential diagnosis
• Management
• Follow up
• References
3.
Introduction
• Definition: Irritabilityin children = excessive crying,
fussiness, or distress disproportionate to the situation.
• Common in infants and young children; can signal
underlying medical, environmental, or psychological
issues.
• Early identification critical to address potentially serious
conditions (e.g., infections, pain, neurological issues).
4.
Epidemiology
• Studies havereported a percentage of all annual ED visits for infant
crying ranging from 0.25% to 13.6%
5.
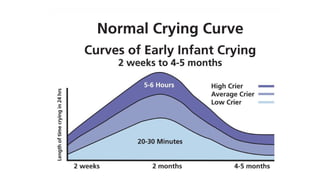
How much doesa baby cry?
• Normal infant crying follows typical pattern in otherwise healthy
infants
• Progressively increases after2 weeks and peaks in second month of
life, then gradually decreases by fourth or fifth month of life
• Peaks in late afternoon and evening within first 6months of life
• May occur for several hours per day
• May be unrelated to needs of infant and therefore difficult to soothe
7.
How much shoulda baby sleep?
• Birth: 16-18
• 3 months: 14-15h
• 6 week- tired after awake for 1.5hours
• 3 month –tired after 2hours
8.
Etiology
Non pathological causes
•Hunger, thirst, tiredness, discomfort
• Separation from mother
• Temperature disturbances in the environment
• Need to clean up
9.
Etiology
Pathological causes ofcrying
• Most of the diseases of neonates, infants and children have
irritability as a major manifestation.
• For pediatrician it is important to decide the cause of
irritability/crying, though difficult at times
ETIOLOGY
(IT CRIES)
• Iinfections (otitis media, sepsis, meningitis, UTI etc)
• T trauma( child abuse, fractures, hair tourniquet etc)
• C cardiac diseases- congenital colic, constipation
• R reflux, rectal/annual fissure
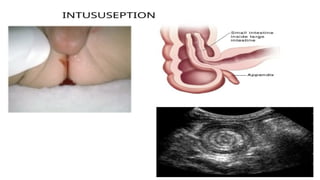
• I intersusception
• E eyes ( corneal abrasion, foreign body, glaucoma
• S skin eg diaper rash. Subdural hematoma
12.
Red flag
• Persistentinconsolability beyond initial assessment
• Sudden increase in frequency or duration of inconsolability
• Ill appearance or abnormal vital signs
• Paradoxical crying(i.e. crying when handled which resolves when left undisturbed
• Unexplained poor growth
• Developmental delay
• Concern for trauma(e.g. fall, physical abuse
• Injury in precruising infants/mobile (i.e. bruises, subconjunctival hemorrhage
• Abdominal tenderness or distension
• Previous or current neurological symptoms of findings( unexplained seizures, apnea,
altered mental status
14.
Clinical Presentation
History
• Onset,duration, and pattern of irritability (constant vs.
episodic). Factors that relieve or exacerbate it
• Associated symptoms: Fever, feeding difficulties, vomiting,
sleep changes.
• Triggers: Feeding, diaper changes, environmental factors.
Recent changes in care arrangements
• Developmental history, recent stressors, or family history of
similar issues.
• Caregiver perception.
16.
Physical Examination
• GeneralAppearance: Assess consolability, alertness, or
lethargy. Note posture (e.g., arched back in pain,
listlessness in sepsis).
• Vital Signs: Check temperature (fever/hypothermia),
heart rate (tachycardia), respiratory rate (distress), and
oxygen saturation.
• Systematic exam critical in resource-limited settings to
prioritize life-threatening conditions (e.g., sepsis,
dehydration).
18.
Physical Examination
• Headand Neck:
• Fontanelles (infants): Bulging (raised intracranial
pressure) or sunken (dehydration).
• ENT: Inspect ears for otitis media (red, bulging tympanic
membrane), throat for tonsillitis, or nasal passages for
foreign bodies.
19.
Physical Examination
• Neurological:Evaluate tone (hyper/hypotonia), reflexes,
and consciousness level (Glasgow Coma Scale if altered).
Look for meningeal signs (e.g., neck stiffness, Kernig’s
sign).
• Abdomen: Palpate for distension, tenderness, or masses
(e.g., intussusception). Auscultate for bowel sounds.
• Skin: Inspect for rashes (e.g., petechiae in meningitis),
bruising (trauma/non-accidental injury), or pallor.
20.
Physical Examination
• Musculoskeletal:Check for limb tenderness, swelling, or
limited movement (e.g., fractures, osteomyelitis).
• Eyes: Assess for corneal abrasions (fluorescein staining),
conjunctivitis, or abnormal pupil response (neurological
concerns).
24.
Diagnosis
• Complaint ofcrying is so nonspecific, differential diagnosis is so
extensive,
• THOROUGH HISTORY, CLINICAL EXAMINATION
• Prioritize clinical assessment
Infantile colic
• Behavioralstate, characterized by unexplained paroxysms of
inconsolable crying, lasting for more than 3 hrs a day & occurring
more than 3 days in a week, for a period of 3 weeks.
• Occurs in 10-25% of infants
• Onset is usually 2-3 wks of age, peaking at 6-8 wks and remitting at
3-4wks
28.
Management
Support/Conservative
• Reassure caregiversif benign cause (e.g., colic).
• Address environmental factors: Soothing techniques (swaddling,
white noise), feeding adjustments.
• Parental support: Education on normal crying patterns
29.
Care giving strategiesfor irritable infants
• As Described by Dr Harvey Karp THE 5 Ss
1. swaddling
2. side or stomach holding
3. Soothing noises(shushing, singing, white noise)
4. Swinging (Slow rhythmic movement)
5. Sucking on a pacifier
30.
Management
Definitive Treatment
• Treatunderlying cause: Antibiotics for infections,
analgesics for pain, surgery for intussusception.
• Pharmacological: Antipyretics for fever, antacids for
GERD (per UpToDate guidelines).
• Multidisciplinary: Involve social workers if non-
accidental injury suspected.
31.
Follow up
• Regularpediatric visits to track growth and
development.
• Red flags: Persistent irritability, developmental delay, or
recurrent episodes warrant further evaluation.
32.
To Note
• Historyand clinical examination ...the most important tools
• No universally recommended lab tests/ imaging studies.....
Individualize the decisions
• Don't miss underlying serious disorder
35.
The References
• Kliegman,R. M., St. Geme, J. W., Blum, N. J., Shah, S. S., Tasker, R.
C., Wilson, K. M., & Behrman, R. E. (2020). Nelson textbook of
pediatrics (21st ed.). Elsevier.
• World Health Organization. (2013). Hospital care for children:
Guidelines for the management of common illnesses with limited
resources (2nd ed.). World Health Organization.
https://www.who.int/publications/i/item/9789241548373
• Freedman, S. B., & Rodean, J. (2024). Crying and irritability in
infants: Evaluation and management. UpToDate. Retrieved August
17, 2025, from https://www.uptodate.com/contents/approach-to-
the-infant-with-excessive-crying.