THE CRYING CHILD
PRESENTERS:SERIAL NUMBER 44, 58 AND 72
MODERATOR: DR. BABA JIBRIN
DEPARTMENT OF PAEDIATRICS
USMANU DANFODIYO UNIVERSITY, SOKOTO
2.
2
Outline
Introduction/definition ofcrying child
Epidemiology
Types of cry
Effect of excessive crying in infants
Why is child crying
Evaluation of a crying child
Conclusion
References
13/12/2021
The Crying Child
3.
3
Introduction
Crying isthe shedding of tears in response to an emotional state, pain, or physical
irritation of the eye
It is the normal physiological response to many stimuli in nonverbal children
In babies, cry has crucial role in soliciting attention and care from adults
A child is a human being between birth and puberty (< 18 years)
Healthy children cry for about 3 hours per day on an average at 6 weeks of age
with the peak occurrence between 3 PM and 11 PM
Incessant crying is one of the common reasons for many emergency visits during
infancy which often lead to considerable parental stress and anxiety
13/12/2021
The Crying Child
4.
4
Epidemiology
The incidencevaries from 1.5% to 11.9% depending on
the case definitions and age group
It is high in infants below 3 months of age and
decreases considerably beyond 6 months of age.
Reported incidence of serious underlying organic
causes is around 5 to 10% in babies with incessant
crying
13/12/2021
The Crying Child
5.
5
Types of cryin children
1. Normal cry
2. Abnormal cry
a. Rhythmic cry
b. Fussy cry
c. Whiny cry
d. Infantile colic/ behavioral cry
e. High pitch cry
13/12/2021
The Crying Child
6.
6
Abnormal cry
Theseare types of babies’ cry that are unusual and
denote abnormality and pathology in the baby, such
as pain or insect bite
It can be:
A high pitch cry or
An incessant or inconsolable cry
13/12/2021
The Crying Child
7.
7
Abnormal cry
A. Rhythmiccry
This is a repetitive pattern of cry where the baby make sounds like “neh”
due to the baby trying to suck and putting the tongue on the roof of the
mouth
It is usually short, low pitched cries that rise and fall
This type of cry denotes hunger
B. Fussy cry
This happens when the baby is not hungry and has been in a single
position for long
They tend to make a fuss with short low pitch cries which can be consoled
by changing their position or giving a new toy. This denote boredom
13/12/2021
The Crying Child
8.
8
Abnormal cry
C. Whinycry
This cry is a nasal cry ,that sounds like they are saying “owh” and look
like a yawn
This type of cry builds in intensity with time
This denotes tiredness and means the baby needs to take a nap
D. Infantile colic/Behavioural cries
This is defined as a paroxysmal crying of more than 3hours a day
occurring for more than 3days a week lasting for more than 3weeks in
an otherwise healthy child who is older than 3 weeks and younger
than 4 months of age
13/12/2021
The Crying Child
9.
9
Abnormal cry
Someconsider colic as a spectrum ranging between normal cry
and a distinct behavioral syndrome
Colic is a diagnosis of exclusion made after careful history taking
and clinical examination and ruling out any organic cause
Colic is the leading of incessant cry
E. High pitch cry
This type of cry pierces the ears , characterized by loud shrieks
accompanied by a baby arching its back and grunting
it means a baby is in pain
13/12/2021
The Crying Child
10.
10
Abnormal cry
Thistype of cry can also be experienced
after a vaccine shot
it is usually fierce but shortlived
F. Incessant/inconsolable cry
This is the type of cry that is difficult to
console
it goes on for a long time with grunts
and stuttering breath after
This type of cry denotes pain and
significant discomfort
Infantile colic is the commonest cause
This type of cry can also be experienced
after a vaccine shot 13/12/2021
The Crying Child
11.
11
Effects Of Excessivecrying in infancy
1. Parental anxiety and depression
2. Parental sleep deprivation
3. Attachment difficulties between infant and children
4. Excessive cry in babies can trigger an episode of
cyanotic spells in patients with TOF, VSD and TGA.
13/12/2021
The Crying Child
12.
12
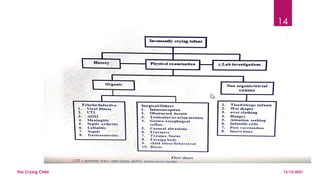
Why is childcrying
The causes are divided into
a) Organic
1. Viral illness
2. UTI
3. Meningitis
4. AOM
5. Septic arthritis
6. Cellulitis
7. sepsis
b) Non-organic/trivial cause
1. Hunger
2. Wet diaper
3. Tiredness/sleepiness
4. Attention seeking
5. Infantile colic
6. Overclothing
7. Insect bite/post vaccination
13/12/2021
The Crying Child
15
Evaluation of acrying child
History
Physical examination
Investigations
Treatment
13/12/2021
The Crying Child
16.
16
Evaluation of acrying child
History
Comprehensive history taking and physical examination should
be the cornerstone in approaching a crying infant
Duration
Frequency
Periodicity and
Intensity of crying episodes
Aggravating and alleviating factors should be recorded
13/12/2021
The Crying Child
17.
17
Evaluation of acrying child
A good History should also focus on
Age
comorbid medical conditions
sibling and family history
recent vaccination
photophobia, feeding and sleeping behaviour
It is also important to assess the mother – infant relationship,
maternal fatigue and stress
Parents are excellent observers and are often able to find subtle
signs and symptoms
13/12/2021
The Crying Child
18.
18
Evaluation of acrying child
Physical examination.
Physical examination ascertains whether the child is
healthy or ill- looking
Vital signs should be recorded and the entire body,
including genitals, should be thoroughly inspected
Eyelids have to be everted for ocular foreign bodies
Infants who continue to cry throughout the initial
assessment should be observed further and re-
examined during normal periods
13/12/2021
The Crying Child
19.
19
Evaluation of acrying child
For example
high pitched incessant cry may indicate central nervous
system infection.
A continuous cry associated with grunting may indicate
respiratory infection / foreign body.
Screaming with pulling at the ears may indicate AOM
Intermittent bouts of crying associated with pallor, with the
knees drawn up over the abdomen may indicate
intussusception
Paroxysmal crying episodes in an otherwise healthy infant less
than 4 months of age typically occurring in the late
afternoon and evening suggest infantile colic
13/12/2021
The Crying Child
20.
20
Evaluation of acrying child
Detailed observation of cry often gives diagnostic clues
Physical examination should be systematic including
head to foot examination
Some parts of examination may be repeated if required
as examining a fussy infant is not easy
13/12/2021
The Crying Child
21.
21
Evaluation of acrying child
Investigations
The clinical assessment should guide decision making about sequential
investigations.
The yield of the laboratory investigations vary with the context of
screening test or confirmation test.
1. Corneal fluorescence test; for screening for corneal abrasion
2. Abdominal ultrasound; intussusception
3. blood cultures; sepsis
4. Urine MCS
5. Stool MCS
6. Gastric washout
7. Ear swab MCS 13/12/2021
The Crying Child
22.
22
Treatment
Crying isa 'common denominator’ for a variety of illnesses and
physiological disturbances
Management of these incessant crying episodes will depend on the
diagnosis obtained
Ruling out apparent causes of crying such as hunger, sleepiness and
tiredness is the first step in treating an infant with persistent crying
In febrile crying infants with or without a focus of infection, the
management should be based on any standard guidelines for sepsis
work up.
Other surgical and miscellaneous conditions should be managed
accordingly.
13/12/2021
The Crying Child
23.
23
Treatment
Treatment strategiesfor infant colic include drugs, dietary
modifications and behavioral interventions.
Behavioral interventions should be tried first as it has documented
efficacy.
If they fail to produce relief, drug and dietary management may
be tried.
Dicyclomine has been shown to effectively reduce infant crying in
two randomized controlled trial
13/12/2021
The Crying Child
24.
24
Treatment
Supportive careis very essential when no underlying medical
cause is found
Mother’s emotional state and the mother–baby relationship should
be addressed
Ensure that the baby is adequately fed and rested. Some general
measures such as firmly holding the baby, swaddling, massaging,
singing and playing white noise may be tried
White noise has a soothing effect on crying and irritable infants
13/12/2021
The Crying Child
25.
25
Prevention
General healthpromotion and health education.
Specific protection- immunisation .
Treatment of specific disease.
Limitation of disability
Rehabilitation
13/12/2021
The Crying Child
26.
26
Conclusion
Crying isa normal part of your baby’s development
and is normal for all babies from all cultural
backgrounds
An inconsolable cry without any obvious causes such as
hunger, thirst, loneliness, wet diaper, loud noise, requires
detailed search for a medical cause
13/12/2021
The Crying Child
27.
27
References
The evaluationand management of an incessantly crying infant
Jayavardhana Arumugam1, S Sivandam2, A M Vijayalakshmi3 Sri
Lanka Journal of Child Health 2012; 41(4): 192-198
Encyclopedia on early childhood education
Kiwix the medical encyclopedia
13/12/2021
The Crying Child
CLINICAL PRESENTATION
• PARALYTICPOLIOMYELITIS
• Is the least common form (<1%)
• It's characterized by descending asymmetric acute flacid paralysis
(AFP)
• Proximal muscles are affected earlier than the distal muscles
• paralysis starts at hip and proceed towards extremities giving rise to
the characteristics tripod sign (child sits with flexed hip, both arms are
extended towards the back for support
32.
The Crying Child
32
13/12/2021
•Sites involved can be spinal, bulbar or
bulbospinal and the nature of paralysis varies
accordingly
• The disease progression is typically biphasic,
aseptic meningitis occurs followed by recovery
and then fever with paralytic features 1-2 days
after
33.
The Crying Child
33
13/12/2021
•Sites involved can be spinal, bulbar or
bulbospinal and the nature of paralysis
varies accordingly
• The disease progression is typically
biphasic, aseptic meningitis occurs
followed by recovery and then fever with
paralytic features 1-2 days after
TREATMENT
• There isno specific antiviral treatment for poliomyelitis
• The management is supportive and aim at limiting progression of the
disease
• All intramuscular injections and surgical procedures are
contraindicated during the acute phase of the disease especially in
the first week of the illness as they might result in the progression of
disease
TREATMENT
• ABORTIVE POLIOMYELITIS
•Supportive treatment with analgesics, sedatives and bed rest untill
child's temperature is normal
• Careful neurologic and musculoskeletal examination should be
performed 2 months later to detect any minor involvement
TREATMENT
• NONPARALYTIC POLIOMYELITIS
•Similar to that of avortive form
• Analgesics for relief for the discomfort of muscle tightness and spasm
of the neck, trunk and extremities
• Hot packs for 15-30 minutes every 2-4 hours
• Hot tube bath and firm bed
• Patient should be carefully examined every 2 months after apparent
recovery to detect minor residual effect that may cause postural
problems in later years
• PARALYTIC POLIOMYELITIS
•Mechanical ventilation is often needed in
• patients with bulbar paralysis. Tracheostomy care is
• often needed in patients requiring long-term ventilatory
• support. Phys ical therapy is indicated in cases of
• paralytic disease. In paralytic disease, provide frequent
• mobilization to avoid development of chronic decubitus
• ulcerations. Active and passive motion exercises are
• indicated during the convalescent stage.
e. Faecal
• impactionis frequent in cases of paralytic disease and
• can be treated with laxatives as soon as it develops. A
• multidisciplinary approach with the Phys iotherapist,
• Pulmonologist, Neurologist, Immunologist, and
• Infectious Diseases Specialist is essential.
• Diet: Patients with poliomyelitis are prone to develop
• constipation, therefore a diet rich in fibre is usually
• indicated.
• Other supportive care: Patients with poliomyelitis may
• develop bladder dysfunction for which catheterization is
• frequently required or manual compression of the
• bladder.
• Prevention; Two types of vaccines
44.
The Crying Child
44
13/12/2021
•GENERAL HEALTH PROMOTION
• Health education
• Environmental sanitation
• Personal hygiene
• SPECIFIC PROTECTION
• ..
Editor's Notes
#21 If there are no clues in the patient's history or by physical
examination suggesting a specific infection or area of suspicion, it is unlikely that diagnostic studies will be helpful in identifying the aetiology. A period of observation or follow up would be desirable in those cases till diagnosis is established. At times negative results help in ruling out serious illness and for reassurance before discharge.
#23 Risk of apnoea and seizures should be considered before recommending dicyclomine
#24 . Parents and care givers should be given an explanation about normal crying and sleep patterns, and to recognize needs and discomforts of the baby