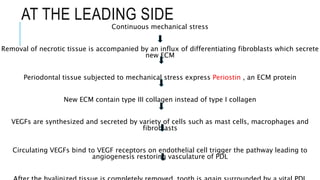
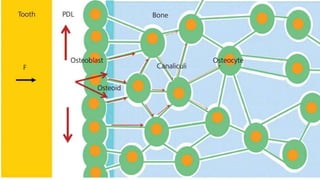
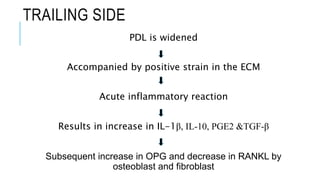
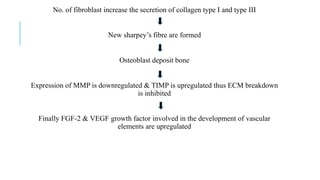
The document discusses the cellular biological processes involved in orthodontic tooth movement, detailing the phases of hyalinization and bone resorption. It explains how mechanical stress impacts periodontal fibroblasts and osteoclasts, highlighting the role of various cytokines and enzymes in these processes. Additionally, the document emphasizes the interactions between different cellular precursors and the extracellular matrix during tooth movement.












































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)



