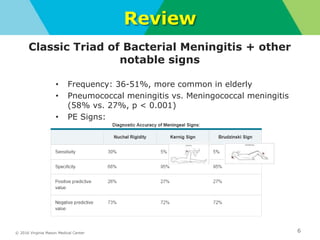
The document discusses a noon conference presentation on bacterial meningitis. It includes a review of CSF findings in bacterial meningitis versus viral meningitis. It also reviews the classic triad of bacterial meningitis and other notable signs and symptoms. Empiric antibiotic coverage for various pathogens is discussed. Guidelines on when to perform lumbar puncture versus CT are provided. Multiple choice questions from MKSAP and NEJM Knowledge+ are reviewed covering topics like adjuvant dexamethasone use, antibiotic coverage for different populations, and nosocomial meningitis.

























































![2019 04-30 noon conference [stephen slade]](https://cdn.slidesharecdn.com/ss_thumbnails/2019-04-30noonconferencestephenslade-190501212611-thumbnail.jpg?width=640&height=640&fit=bounds)



























