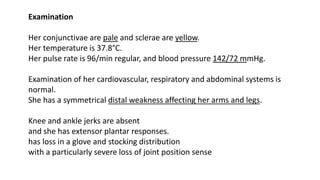
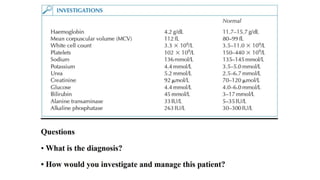
A 63-year-old woman presented with fatigue, breathlessness, lightheadedness, and numbness in her feet. On examination, she had pale conjunctiva, increased heart rate, absent reflexes, and loss of sensation in her extremities. Testing revealed macrocytic anemia, low vitamin B12 levels, and antibodies associated with pernicious anemia. She was diagnosed with megaloblastic anemia due to vitamin B12 deficiency from pernicious anemia. She received injections of hydroxycobalamin and will continue injections every 3 months for management.






















![BLOOD_DISORDERS-2[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/blooddisorders-21-230610142333-f4472c75-thumbnail.jpg?width=640&height=640&fit=bounds)

























