Downloaded 55 times

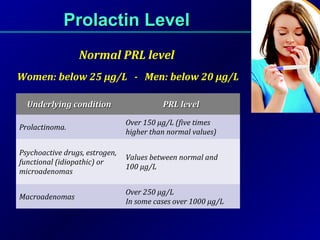

















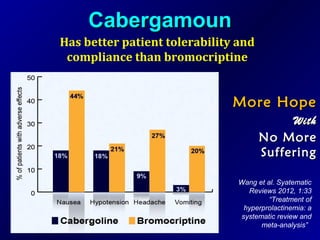












Prolactin enhances breast development during pregnancy and induces lactation. It is produced in the pituitary gland and its levels are normally inhibited by dopamine. Prolactin levels may be elevated in conditions like prolactinomas or certain drugs. Hyperprolactinemia can cause symptoms like menstrual irregularities, infertility, and galactorrhea. Prolactinomas are treated initially with dopamine agonists like cabergoline, which lower prolactin levels by activating D2 receptors on lactotroph cells. Cabergoline is more potent and long-acting than bromocriptine, making it a preferred treatment for conditions involving elevated prolactin levels.











































































