INTRODUCTION
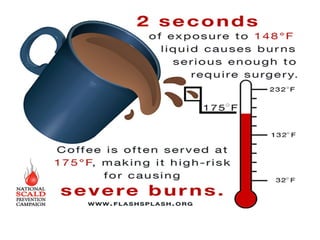
A burn occurswhen there is injury to the tissues of
the body caused by heat, chemicals, electric current
or radiation. The resulting effects are influenced by
the temperature of the burning agent, duration of
contact time and type of tissue that is injured.
10.
DEFINITION
A burn isan injury to the skin or other organic
tissues primarily caused by heat or due to
radiation, radioactivity, electricity, friction or
contact with chemicals.
11.
INCIDENCE
According to WHO
•Burns are a global public health problem accounting
for an estimated 195000 deaths annually. The majority
of these occur in low and middle income countries and
almost half occur in the WHO south-east Asia region
• Non-fatal burn injuries are a leading cause of morbidity
in woman. In the WHO south east Asia region have the
highest rate of burns accounting for 27% of global burn
deaths and nearly 70% o burn deaths in the region
• Burn occurs most commonly in home and workplace
12.
Some country data
•In India
Over 1000000 people are moderately or several burnt
every year in India.
• Nearly 173000 Bangladesh children are moderately or
severely bunt every year.
• In Colombia, Egypt and Pakistan 17% of children with
burns have a temporary disability and 18% have
permanent disability.
• Burns are the second most common injury in rural Nepal
accounting for 5% of disabilities.
• IN 2008, OVER 410000 Burn injuries occurred in the
USA with approximately 40,000 requiring hospitalization.
13.
COMMON PLACES ANDCAUSES OF BURN INJURY
1) Occupational Hazards
Tar
Chemicals
Hot metals
Steam pipes
Combustible fuels
Fertilizers/ pesticides
Electricity from power lines
Sparks from live electric sources
14.
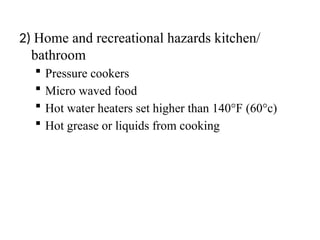
2) Home andrecreational hazards kitchen/
bathroom
Pressure cookers
Micro waved food
Hot water heaters set higher than 140°F (60°c)
Hot grease or liquids from cooking
15.
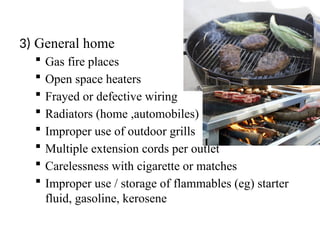
3) General home
Gas fire places
Open space heaters
Frayed or defective wiring
Radiators (home ,automobiles)
Improper use of outdoor grills
Multiple extension cords per outlet
Carelessness with cigarette or matches
Improper use / storage of flammables (eg) starter
fluid, gasoline, kerosene
16.
RISK FACTORS (WHO)
a)Gender
Females suffer burns more frequently than males. High
risk in females is associated with open fire cooking or
inherently unsafe cook stores which can ignite loose
clothing open flames used for heating and lighting, self
directed or interpersonal violence.
b)Age
Along with adult woman children are particularly
vulnerable to burns. Burns are 11th
leading cause of
death of children aged 1-9 years and are also the 5th
most common cause of non fatal childhood injuries.
17.
c)Regional factors
Infantsin the African Region have 3 times the
incidence of burn deaths than infants world wide
Boys under five years of age living in low and
middle income countries have twice as likely
chance of burn death than boys living in high
income countries.
d) Socio Economic Factors
People living in low and middle income
countries are at high risk of burns than people
living in high income countries.
18.
e) Other riskfactors
Occupations that increases exposure to fire
Poverty, overcrowding
Lack of proper safety measures
Placement of young girls in household roles
such as cooking and care of small children
Underlying medical conditions including
epilepsy, peripheral neuropathy and
physical and cognitive disabilities
19.
Alcohol abuse andsmoking
Easy access to chemicals used for
assault (e.g.) acid for violence
attacks
Inadequate safety measures for
liquid fuel petroleum gas and
electricity
20.
TYPES OF BURNINJURY
1. Chemicals burns
2. Smoke and inhalation injury
Types of smoke and inhalation injuries:
Carbon monoxide poisoning:
Inhalation injury above the glottis
Inhalation injury below the glottis
Chemicals burns
Chemicals burnsresult from tissue injury and
destruction from acids, alkalis and organic compounds.
Acids are found in many household cleaners and include
HCL, oxalic and hydro fluorine acid. Alkalis adhere to
tissue causing protein hydrolysis and liquid faction. This
damage continues even when the alkali is neutralized.
Alkalis are found in oven and drain cleaners, fertilizers,
heavy industrial cleaners.
23.
• Organic compoundsincluding phenols and petroleum
products produce contact burns and system toxicity.
Phenols are found in chemical disinfectants, petroleum
products include creosote and gasoline
• When chemical burn occurs it may cause damage to
the skin, eye, respiratory problems may arise and it also
causes system manifestations including involvement of the
liver and kidney
24.
Management of chemicalsburns
• Remove the person from the burning agent and begin to
quickly remove the chemical from the skin
• Dry chemical should be brushed from the skin and the
affected area should be flushed with copious amounts of
water to irrigate the skin. This technique can be effective
anywhere from 20mts to 2 hours post exposure
• Any clothing containing the chemical should be removed.
• Tissue destruction may continue for up to 72 hours after a
chemical injury
25.
Smoke and inhalationinjury
Smoke and inhalation injuries results from the
inhalation of hot air or noxious chemicals and can
cause damage to the tissues of the respiratory tract. In
this type of injury redness and airway swelling edema
may occur.
Types of smoke and inhalation injuries
There are three types of smoke and inhalation injuries:
• Carbon monoxide poisoning:
• Inhalation injury above the glottis
• Inhalation injury below the glottis
26.
• Presence offacial burns
• Singed nasal hair
• Hoarseness
• Painful swallowing
• Dark oral & nasal mucous membrane
• Carbonaceous sputum
• Burns around the chest and neck & history of
burns in enclosed space
27.
Thermal Burns
Thermal burnsmay be caused by
flame, flash or hot liquids or contact with
hot objects such as hot cooking pan, sun
burn(Radiation burn).
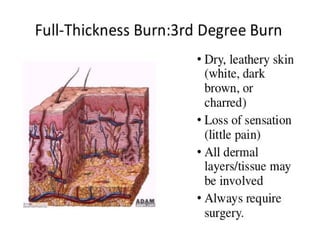
• Painless withno sensation to touch
• Skin is pearly white or charred, dry and may
appear leathery
32.
Risk reduction strategiesfor flame injury
• Never leave candles un attended near open
windows or curtains
• Encourage use of child resistant lighters
• Install smoke or carbon monoxide
Detectors
• Encourage use of home fire exit drills
• Never leave hot oil un attended
• Do not smoke in bed.
33.
Risk reduction strategiesfor Scald injury
• Lower hot water temperature to the lowest point
(120 degree F or 40 degree celsius)
• Utilize anti scald devices with shower head .
• Supervise bathing with small children or older
adults or the one with disabilities
• Check temperature of the hot water with back of
the hand always.
• Exercise caution in use of micro waved food and
beverages
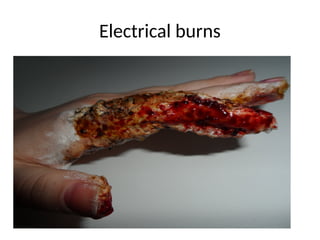
Electrical Burns
Occurs dueto Intense heat generated
from an electric current causes
direct damage to the nerves & blood
vessels tissue anoxia and death.
38.
The severity ofdamage depends on
the amount of voltage, tissue resistance,
current path ways, surface area in contact
with the current and the length of the
time current flow was sustained.
39.
• Dysarrhythmias orCardiac arrest
• Severe Metabolic acidosis and myoglobin
release into the circulation
• Myoglobinuria
• Acute tubular necrosis & ARF
&
Cardiac standstill or fibrillation, Fracture
40.
Management
• Identify theseverity of electric shock
• Complete assessment of the patient
• Transfer to burn unit
• Cervical spine immobilization
• CPR
• Cardiac monitoring
41.
• ABG assessment
•Fluid resuscitation immediately with sodium
bicarbonate to maintain sr. PH level
• ATN-RL-to maintain Urine output of
75-100ml/hour
• Osmotic Diuretic (Mannitol)
42.
Cold thermal injury(Frost bite/True tissue
freezing)-Formation of ice crystals in the tissues
• Peripheral vasoconstriction
• Decreases blood flow
• Vascular stasis
• Cellular temp decreases
• Intracellular sodium and chloride increases
• Cell membranes destroyed, Organelles are
damaged
• edema
43.
Types
• Superficial-Skin &subcutaneous tissues
(ear,nose,fingers& toes ).Skin appears-
waxy pale yellow to blue to mottled –
crunchy & frozen-Tingling,numbness or
burning sensation,blisters
44.
Treatment
• Clothing &jewellery should be removed
• The affected extremity should be immersed in
a water bath (102-108F)
• Warm soaks –face
• Blisters-debrided and sterile dressing is
applied
• Analgesics
• T.T Prophylaxis
45.
• Deep –Muscles,bone & tendon.Skin-
white,hard and insensitive to
touch.Appearance of deep thermal
injury with mottling-Gangrene
46.
Treatment
• The affectedextremity should be immersed in
a water bath (102-108F)
• Re warm the extremity and elevate them to
reduce edema
• I.V analgesics
• T.T prphylaxis
• Amputation
47.
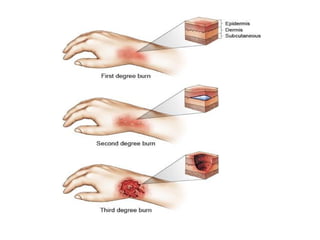
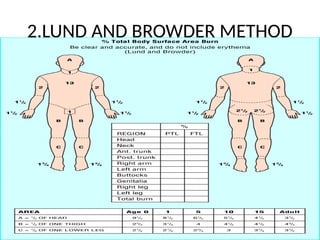
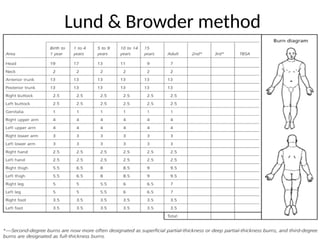
CLASSIFICATION OF BURNINJURY
Burn injuries are classified based on the depth of the
injury and the extent of body surface area injured.
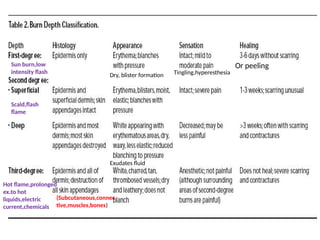
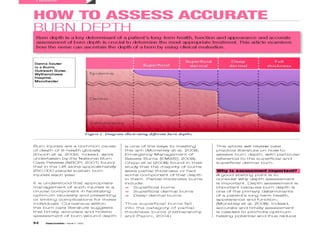
BURN DEPTH
The burn depth depends on the type of injury
Causative agent
Temperature of the burning agent
Duration of contact
Thickness of the skin
48.
CLASSIFICATION OF BURNINJURY
Burns are classified according to the depth of tissue
destruction as,
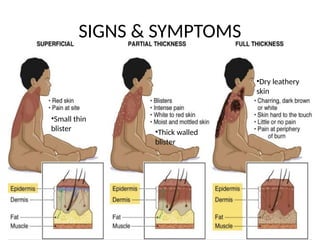
Superficial partial thickness (I Degree)
Deep partial thickness(II Degree)
Full thickness injuries(III Degree)
50.
Dry, blister formationTingling,hyperesthesia
Or peeling
Sun burn,low
intensity flash
Scald,flash
flame
Exudates fluid
(Subcutaneous,connec
tive,muscles,bones)
Hot flame,prolonged
ex.to hot
liquids,electric
current,chemicals
52.
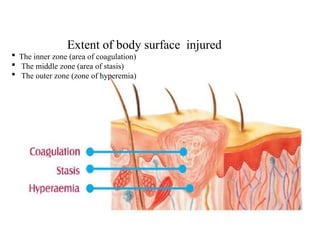
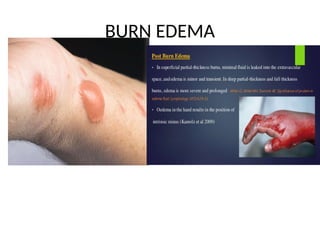
Extent of bodysurface injured
• Area of coagulation: where cellular death
occurs and it sustains the most damage
• Area of stasis : This area has compromised
blood supply, inflammation & tissue injury
• Zone of hyperemia : This is the area of least
damage
53.
Extent of bodysurface injured
The inner zone (area of coagulation)
The middle zone (area of stasis)
The outer zone (zone of hyperemia)
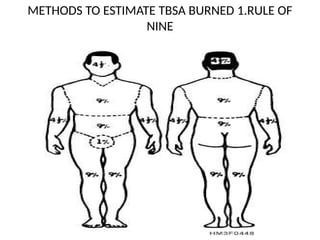
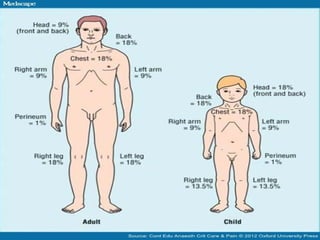
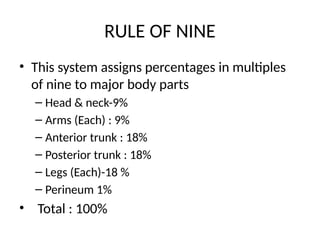
RULE OF NINE
•This system assigns percentages in multiples
of nine to major body parts
– Head & neck-9%
– Arms (Each) : 9%
– Anterior trunk : 18%
– Posterior trunk : 18%
– Legs (Each)-18 %
– Perineum 1%
• Total : 100%
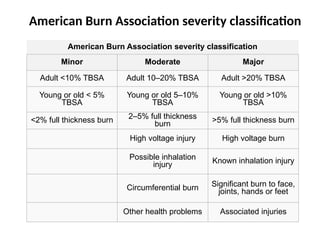
American Burn Associationseverity classification
American Burn Association severity classification
Minor Moderate Major
Adult <10% TBSA Adult 10–20% TBSA Adult >20% TBSA
Young or old < 5%
TBSA
Young or old 5–10%
TBSA
Young or old >10%
TBSA
<2% full thickness burn 2–5% full thickness
burn >5% full thickness burn
High voltage injury High voltage burn
Possible inhalation
injury Known inhalation injury
Circumferential burn Significant burn to face,
joints, hands or feet
Other health problems Associated injuries
EFFECTS ON FLUID,ELECTROLYTESAND
BLOOD VOLUME
Burn Shock, Evoporation of fluid through the burn
wound
Decreased circulatory fluid volume
• Sodium level decreases due to sodium depletion
• Hyperkalemai due to massive cell depletion
• RBC damage-----Anemia------Hypoxemia
• Elevated hematocrit due to plasma loss
• Prolonged clotting & Prothrombine time due to
decreased platelet
68.
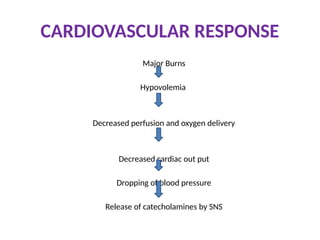
PULMONARY RESPONSE
Pulmonary edemaand airway obstruction
Decreased alveolar exchange
Hyperventilation and increased oxygen
consumption
Respiratory alkalosis due to hyperventilation and
later respiratory acidosis due to pulmonary
insufficiency
69.
METABOLIC DEMANDS
• Hypermetabolism due to catecholamine release
• Burn fever (102-103)
• Gluconeogenesis due to increased glucose
demand and exhaustion of glucose stores
• Decreased insulin level------Hyperglycemia
• Mobilization of skeletal and visceral proteins
Weight loss
Development of Negative Nitrogen Balance
70.
So the patientneed
• 3000-5000kcal or more/day
• Burn of less than 10% needs minimal
supplementation
• High protein high calorie diet is needed for 12-
20% burns
• Between20 and 30% -enternal feedigs
• TBSA burns of 30-40% require TPN
71.
RENAL CHANGES
Decreased GFR
DecreasedRenal blood flow
High output or oliguria,renal failure,decreased
creatinine clearance
Presence of Hb and myoglobin in urine
Acute tubular necrosis
72.
IMMUNOLOGIC ACTIVITY
• Lossof skin barrier and presence of eschar favors bacterial
growth
Abnormal inflammatory response
Decreased delivery of WBC and oxygen to the injured area
Hypoxia, acidosis and thrombosis of vessels, , Lymphocytopenia,
Decreased immunoglobulins and sr.Albumin
• Depressed cellular immunity, Impaired host resistance
Burn wound sepsis
Septicemia
,
73.
G I IMPACT
MajorBurns
SNS response
Decreased peristalsis
Gastric distension,nausea,vomiting,paralytic
ileus
Decreased blood flow to G I tract vessels
Ischemia & Gastric ulcer
Occult bleeding, life threatening hemorrhage
















































![Common neonatal problems [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/commonneonatalproblemsautosaved-251112045426-cb3b06ad-thumbnail.jpg?width=640&height=640&fit=bounds)











![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













