- 32 year old female diagnosed with triple negative breast cancer and admitted for MRM surgery.
- She previously underwent lumpectomy which showed invasive ductal carcinoma.
- She received 4 cycles of neoadjuvant chemotherapy and was scheduled for MRM.
- Physical exam and tests showed no signs of metastasis.
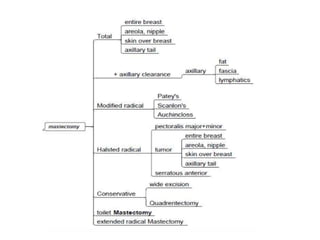
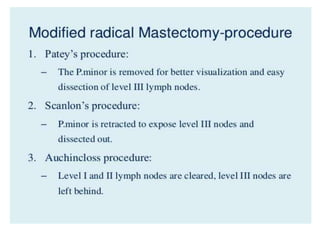
- She underwent MRM surgery which included removal of breast tissue and axillary lymph nodes.