Brachial Plexus Anatomy
•Download as PPTX, PDF•
1 like•82 views

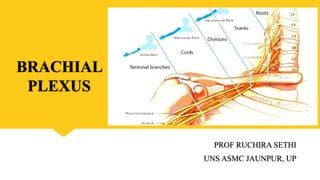
The brachial plexus is formed by the anterior rami of cervical spinal nerves C5-T1. It has roots, trunks, divisions, cords, and terminal branches that provide motor and sensory innervation to the upper limb. Injuries can cause conditions like Erb's palsy or Klumpke's paralysis. The brachial plexus can also be blocked for anesthesia of the upper extremity.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Brachial Plexus Anatomy
Similar to Brachial Plexus Anatomy (20)
Recently uploaded
Recently uploaded (20)
Brachial Plexus Anatomy
- 1. BRACHIAL PLEXUS PROF RUCHIRA SETHI UNS ASMC JAUNPUR, UP
- 2. LEARNING OBJECTIVES • To learn about location and formation of brachial plexus • To discuss the components of brachial plexus • To discuss about Erb’s point & palsy • To learn about the deformity produced in Klumpke’s paralysis • To discuss various other clinical aspects of the plexus
- 3. Structure of a Typical Spinal Nerve
- 4. Scalene group of muscles Scalenus anterior Scalenus medius Scalenus posterior Innervated by cervical spinal nerves
- 5. Formation: anterior primary rami of C5,C6,C7,C8 & T1 spinal nerve, in the neck. • Pre-fixed plexus –C4 • Post –fixed plexus—T2
- 6. Components: Roots C5,C6,C7,C8,T1 Located in neck behind scalenus anterior Trunks Upper trunk Middle trunk Lower trunk Located in lower part neck between cleft of s.anterior & medius Divisions Anterior division(3) Posterior division (3) Located behind clavicle Cords Lateral cord Medial cord Posterior cord Located under clavicle, posterior to subclavian artery Terminal branches Musculocutaneous Axillary Ulnar Median Radial In arm , forearm & hand Innervation Cutaneous innervation & motor supply to complete upper limb
- 7. Relations of Brachial Plexus • Trunks lie in neck; lower trunk posterior to artery while upper and middle behind the subclavian artery • Divisions enter axilla through cervico- axillary canal • Cords & branches form the infraclavicular part of plexus • Cords are in relation to axillary artery
- 8. Relations of axillary artery First part axillary artery Second part axillary artery
- 9. Third part axillary artery
- 11. Branches of Roots: 1. Nerve to serratus anterior or long thoracic nerve of Bell (C5-C7) 2. Nerve to rhomboideus major & minor (dorsal scapular nerve) (C5) 3. Branches to longus colli & scalene group of muscles (C5-C8) 4. Phrenic nerve (C5)
- 12. Branches from trunks From Upper trunk Suprascapular nerve- for supraspinatus & infraspinatus Nerve to subclavius- for subclavius Erb’s point
- 13. Branches from Cords From Lateral cord 1. Lateral pectoral nerve 2. Musculocutaneous n 3. Lateral root of median nerve From Posterior cord 1. Lower subscapular nerve 2. Upper subscapular nerve 3. Nerve to latissimus dorsi 4. Axillary nerve 5. Radial nerve From Medial cord 1. Medial pectoral nerve 2. Medial cutaneous nerve of arm 3. Medial cutaneous nerve of forearm 4. Ulnar nerve 5. Medial root of median nerve
- 14. Applied Aspects of Brachial Plexus 1. Erb’s paralysis (injury to upper brachial plexus) 2. Klumpke’s paralysis (injury to lower brachial plexus) 3. Horner’s syndrome 4. Brachial plexus nerve block
- 15. Cutaneous innervation of the upper limb
- 18. Erb’s Paralysis 1. At Erb’s point 2. Excessive increase between head & shoulder 3. Policemen tip hand 4. Shoulder adducted and medially rotated 5. Elbow extended 6. Forearm pronated
- 20. Klumpke’s Paralysis 1. Lower trunk injury 2. Upward traction (forced abduction) 3. Involves C8,T1 4. Characteristic Claw hand 5. Fingers hyperextendedat MCP joint & flexed at IP joint 6. Adduction & abduction of fingers is lost 7. Sensory loss over medial side of arm forearm and hand
- 23. Horner’s syndrome If T1 is injured proximal to white rami communicantes to first thoracic sympathetic ganglion
- 26. Brachial Plexus Block • Blockade of the brachial plexus is an effective method for providing anesthesia to the upper limb from the shoulder to the fingertips • Interscalene brachial plexus block: anesthesia to the from the distal extent of the clavicle, shoulder joint, and proximal humerus • Superior trunk block: provides analgesia to the shoulder capsule and proximal humerus. diaphragm sparing modification of the interscalene block. • Supraclavicular brachial plexus block: anesthesia of the upper limb from the mid humerus to the fingertips. • Infraclavicular brachial plexus block: anesthesia of the upper limb from the mid- humerus to the fingertips. This block typically spares the intercostobrachial nerve. • Axillary brachial plexus block: anesthesia of the upper limb from mid humerus to the fingertips. This block also spares the intercostobrachial nerve,